Centre for Maternal and Newborn Health, Liverpool School of Tropical Medicine, Liverpool, United Kingdom.
PLoS One. 2019 May 9;14(5):e0215864. doi: 10.1371/journal.pone.0215864. eCollection 2019.
To identify the causes and categories of stillbirth using the Application of ICD-10 to Deaths during the Perinatal Period (ICD-PM).
Prospective, observational study in 12 hospitals across Kenya, Malawi, Sierra Leone and Zimbabwe. Healthcare providers (HCPs) assigned cause of stillbirth following perinatal death audit. Cause of death was classified using the ICD-PM classification system.
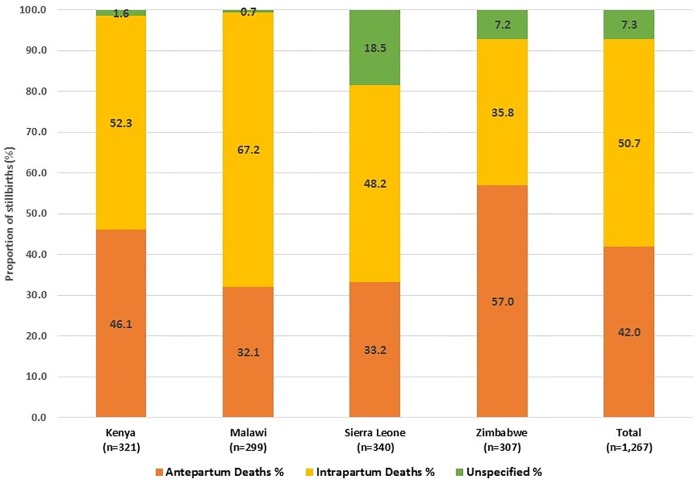
1267 stillbirths met the inclusion criteria. The stillbirth rate (per 1000 births) was 20.3 in Malawi (95% CI: 15.0-42.8), 34.7 in Zimbabwe (95% CI: 31.8-39.2), 38.8 in Kenya (95% CI: 33.9-43.3) and 118.1 in Sierra Leone (95% CI: 115.0-121.2). Of the included cases, 532 (42.0%) were antepartum deaths, 643 (50.7%) were intrapartum deaths and 92 cases (7.3%) could not be categorised by time of death. Overall, only 16% of stillbirths could be classified by fetal cause of death. Infection (A2 category) was the most commonly identified cause for antepartum stillbirths (8.6%). Acute intrapartum events (I3) accounted for the largest proportion of intrapartum deaths (31.3%). In contrast, for 76% of stillbirths, an associated maternal condition could be identified. The M1 category (complications of placenta, cord and membranes) was the most common category assigned for antepartum deaths (31.1%), while complications of labour and delivery (M3) accounted for the highest proportion of intrapartum deaths (38.4%). Overall, the proportion of cases for which no fetal or maternal cause could be identified was 32.6% for antepartum deaths, 8.1% for intrapartum deaths and 17.4% for cases with unknown time of death.
Clinical care and documentation of this care require strengthening. Diagnostic protocols and guidelines should be introduced more widely to obtain better data on cause of death, especially antepartum stillbirths. Revision of ICD-PM should consider an additional category to help accommodate stillbirths with unknown time of death.
利用《国际疾病分类第十次修订本用于围产期死亡(ICD-PM)应用》确定死产的原因和类别。
在肯尼亚、马拉维、塞拉利昂和津巴布韦的 12 家医院进行前瞻性、观察性研究。医疗保健提供者(HCPs)在围产期死亡审核后确定死产原因。使用 ICD-PM 分类系统对死因进行分类。
符合纳入标准的死产 1267 例。死产率(每 1000 例活产)分别为马拉维 20.3(95%CI:15.0-42.8)、津巴布韦 34.7(95%CI:31.8-39.2)、肯尼亚 38.8(95%CI:33.9-43.3)和塞拉利昂 118.1(95%CI:115.0-121.2)。在纳入的病例中,532 例(42.0%)为产前死亡,643 例(50.7%)为产时死亡,92 例(7.3%)无法按死亡时间分类。总体而言,只有 16%的死产可以通过胎儿死因进行分类。感染(A2 类)是产前死产最常见的原因(8.6%)。急性产时事件(I3)占产时死亡的比例最大(31.3%)。相比之下,76%的死产可以确定与母亲相关的情况。M1 类别(胎盘、脐带和胎膜并发症)是产前死亡最常见的类别(31.1%),而分娩和分娩并发症(M3)占产时死亡的比例最高(38.4%)。总体而言,产前死亡、产时死亡和未知死亡时间的病例中,无法确定胎儿或母亲原因的比例分别为 32.6%、8.1%和 17.4%。
需要加强临床护理和护理记录。应更广泛地引入诊断方案和指南,以获得更好的死因数据,特别是产前死产。应修订 ICD-PM,以增加一个额外类别,以帮助容纳未知死亡时间的死产。