Department of Obstetrics and Gynaecology, Federal Teaching Hospital Gombe, Gombe, Nigeria.
African Population and Health Policy Initiative, Gombe, Gombe State, Nigeria.
BMC Pregnancy Childbirth. 2020 Jul 1;20(1):383. doi: 10.1186/s12884-020-03059-8.
Lack of a unified and comparable classification system to unravel the underlying causes of stillbirth hampers the development and implementation of targeted interventions to reduce the unacceptably high stillbirth rates (SBR) in sub-Saharan Africa. Our aim was to track the SBR and the predominant maternal and fetal causes of stillbirths using the WHO ICD-PM Classification system.
This was a retrospective observational study in a major referral centre in northeast Nigeria between 2010 and 2018. Specialist Obstetricians and Gynaecologists assigned causes of stillbirths after an extensive audit of available stillbirths' records. Cause of death was assigned via consensus using the ICD-PM classification system.
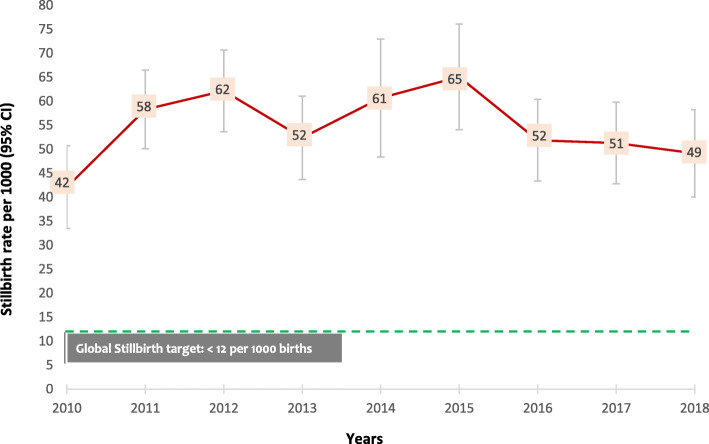
There were 21,462 births between 1 January 2010 and 31 December 2018 in our study setting; of these, 1177 culminated in stillbirths with a total hospital SBR of 55 per 1000 births (95% CI: 52, 58). There were two peaks of stillbirths in 2012 [62 per 1000 births (95% CI: 53, 71)], and 2015 [65 per 1000 births (95% CI, 55, 76)]. Antepartum and intrapartum stillbirths were almost equally prevalent (48% vs 52%). Maternal medical and surgical conditions (M4) were the commonest (69.3%) cause of antepartum stillbirths while complications of placenta, cord and membranes (M3) accounted for the majority (45.8%) of intrapartum stillbirths and the trends were similar between 2010 and 2018. Antepartum and intrapartum fetal causes of stillbirths were mainly due to prematurity which is a disorder of fetal growth (A5 and I6).
Most causes of stillbirths in our setting are due to preventable causes and the trends have remained unabated between 2010 and 2018. Progress toward global SBR targets are off-track, requiring more interventions to halt and reduce the high SBR.
缺乏一个统一和可比的分类系统来阐明死产的根本原因,这阻碍了制定和实施有针对性的干预措施,以降低撒哈拉以南非洲地区高得令人无法接受的死产率。我们的目的是使用世界卫生组织 ICD-PM 分类系统来跟踪死产率以及主要的产妇和胎儿死因。
这是 2010 年至 2018 年在尼日利亚东北部一家主要转诊中心进行的一项回顾性观察研究。妇产科专家在对现有的死产记录进行广泛审核后,确定死产的原因。死因通过 ICD-PM 分类系统的共识来确定。
在我们的研究环境中,2010 年 1 月 1 日至 2018 年 12 月 31 日期间有 21462 例分娩,其中 1177 例最终导致死产,总院内死产率为 55/1000 例(95%CI:52,58)。有两个死产高峰,分别出现在 2012 年[62/1000 例(95%CI:53,71)]和 2015 年[65/1000 例(95%CI:55,76)]。产前和产时死产几乎同样普遍(48%比 52%)。产妇医疗和外科情况(M4)是最常见的产前死产原因(69.3%),而胎盘、脐带和胎膜并发症(M3)占产时死产的大多数(45.8%),这种趋势在 2010 年至 2018 年期间相似。产前和产时胎儿死产的主要原因是早产,这是一种胎儿生长障碍(A5 和 I6)。
在我们的环境中,大多数死产的原因是可预防的,而且 2010 年至 2018 年期间这一趋势没有减弱。在实现全球死产率目标方面进展缓慢,需要采取更多干预措施来阻止和降低高死产率。