Centre for Maternal and Newborn Health, Liverpool School of Tropical Medicine, Pembroke Place, Liverpool, L3 5QA, UK.
BMC Pregnancy Childbirth. 2019 Dec 4;19(1):470. doi: 10.1186/s12884-019-2626-7.
Every year, an estimated 2.6 million stillbirths occur worldwide, with up to 98% occurring in low- and middle-income countries (LMIC). There is a paucity of primary data on cause of stillbirth from LMIC, and particularly from sub-Saharan Africa to inform effective interventions. This study aimed to identify the cause of stillbirths in low- and middle-income settings and compare methods of assessment.
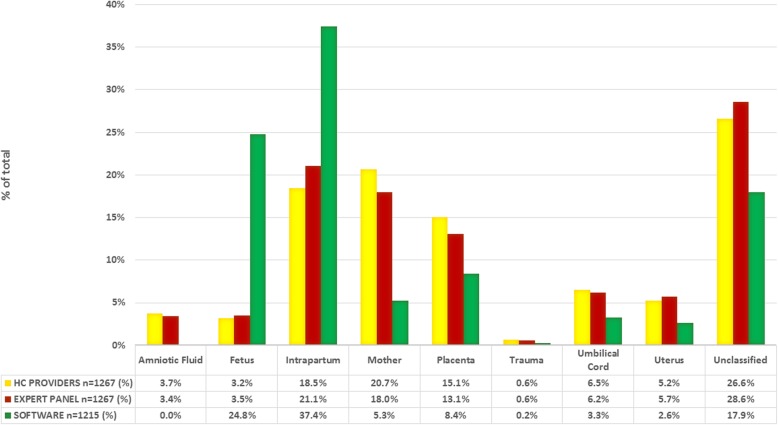
This was a prospective, observational study in 12 hospitals in Kenya, Malawi, Sierra Leone and Zimbabwe. Stillbirths (28 weeks or more) were reviewed to assign the cause of death by healthcare providers, an expert panel and by using computer-based algorithms. Agreement between the three methods was compared using Kappa (κ) analysis. Cause of stillbirth and level of agreement between the methods used to assign cause of death.
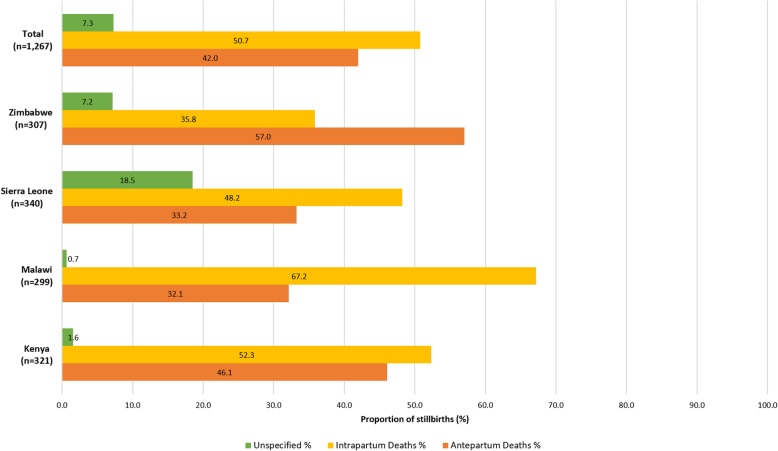
One thousand five hundred sixty-three stillbirths were studied. The stillbirth rate (per 1000 births) was 20.3 in Malawi, 34.7 in Zimbabwe, 38.8 in Kenya and 118.1 in Sierra Leone. Half (50.7%) of all stillbirths occurred during the intrapartum period. Cause of death (range) overall varied by method of assessment and included: asphyxia (18.5-37.4%), placental disorders (8.4-15.1%), maternal hypertensive disorders (5.1-13.6%), infections (4.3-9.0%), cord problems (3.3-6.5%), and ruptured uterus due to obstructed labour (2.6-6.1%). Cause of stillbirth was unknown in 17.9-26.0% of cases. Moderate agreement was observed for cause of stillbirth as assigned by the expert panel and by hospital-based healthcare providers who conducted perinatal death review (κ = 0.69; p < 0.0005). There was only minimal agreement between expert panel review or healthcare provider review and computer-based algorithms (κ = 0.34; 0.31 respectively p < 0.0005).
For the majority of stillbirths, an underlying likely cause of death could be determined despite limited diagnostic capacity. In these settings, more diagnostic information is, however, needed to establish a more specific cause of death for the majority of stillbirths. Existing computer-based algorithms used to assign cause of death require revision.
全球每年估计有 260 万例死产,其中高达 98%发生在中低收入国家(LMIC)。来自 LMIC,特别是撒哈拉以南非洲的关于死产原因的主要数据很少,无法为有效的干预措施提供信息。本研究旨在确定中低收入环境中死产的原因,并比较评估方法。
这是在肯尼亚、马拉维、塞拉利昂和津巴布韦的 12 家医院进行的一项前瞻性、观察性研究。由医疗保健提供者、专家小组以及使用基于计算机的算法对死产(28 周或以上)进行回顾,以确定死亡原因。使用 Kappa(κ)分析比较三种方法之间的一致性。
研究了 1563 例死产。每 1000 例活产中的死产率(‰)分别为马拉维 20.3‰、津巴布韦 34.7‰、肯尼亚 38.8‰和塞拉利昂 118.1‰。一半(50.7%)的死产发生在分娩期间。总体死因(范围)因评估方法而异,包括窒息(18.5-37.4%)、胎盘疾病(8.4-15.1%)、产妇高血压疾病(5.1-13.6%)、感染(4.3-9.0%)、脐带问题(3.3-6.5%)和因梗阻性分娩导致的子宫破裂(2.6-6.1%)。在 17.9-26.0%的病例中,死产原因未知。专家小组评估和进行围产期死亡审查的医院保健提供者对死产原因的评估结果具有中度一致性(κ=0.69;p<0.0005)。专家小组审查或保健提供者审查与基于计算机的算法之间的一致性仅为最小(κ=0.34;0.31,均 p<0.0005)。
尽管诊断能力有限,但对于大多数死产,仍可以确定潜在的死因。然而,在这些环境中,需要更多的诊断信息来确定大多数死产的更具体死因。用于确定死因的现有基于计算机的算法需要修订。