Moncrief Cancer Institute, Fort Worth, Texas.
Moncrief Cancer Institute, Fort Worth, Texas.
Clin Gastroenterol Hepatol. 2020 Mar;18(3):647-653. doi: 10.1016/j.cgh.2019.04.077. Epub 2019 May 11.
BACKGROUND & AIMS: Noninvasive tests used in colorectal cancer screening, such as the fecal immunochemical test (FIT), are more acceptable but detect neoplasias with lower levels of sensitivity than colonoscopy. We investigated whether lowering the cut-off concentration of hemoglobin for designation as an abnormal FIT result increased the detection of advanced neoplasia in a mailed outreach program.
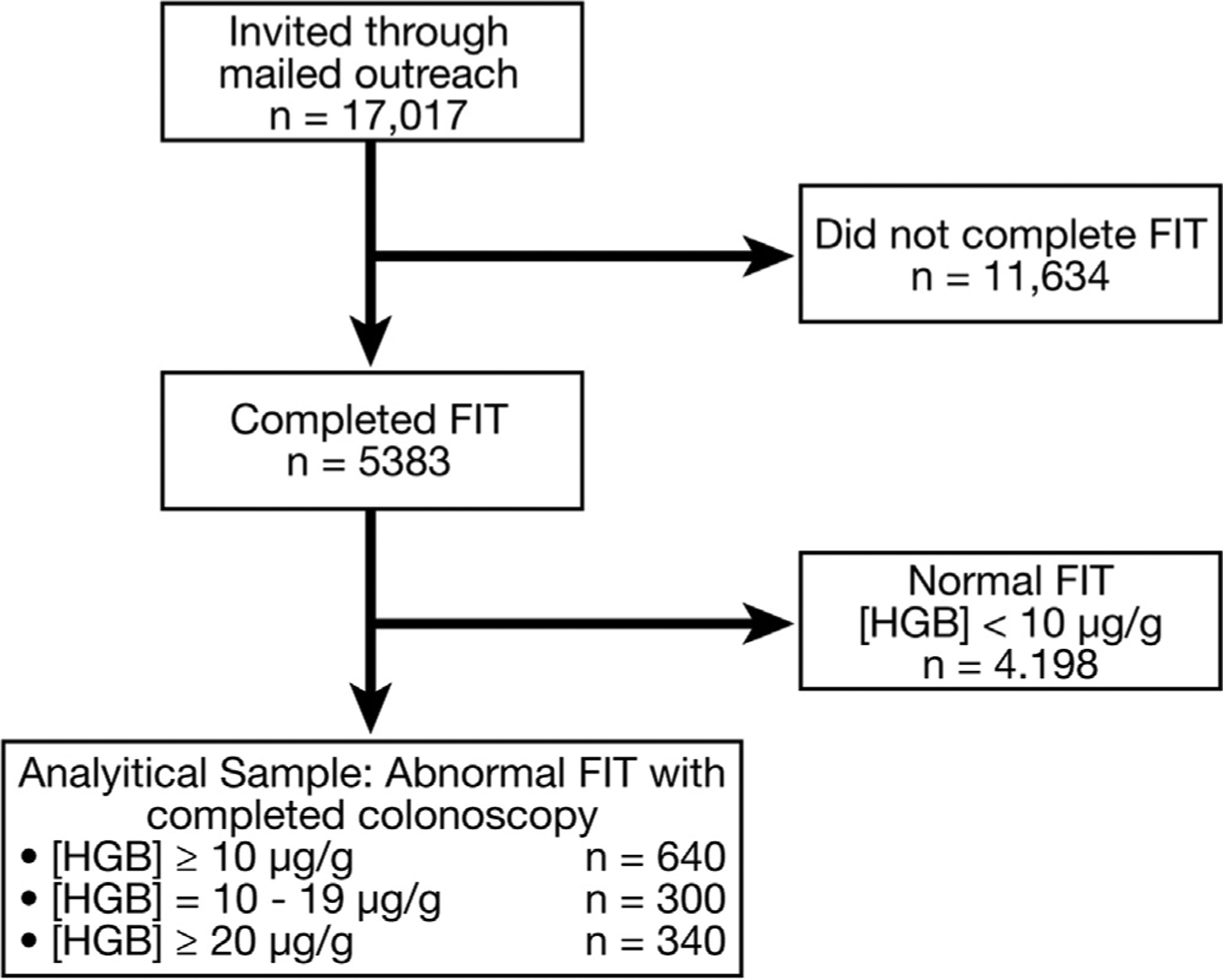
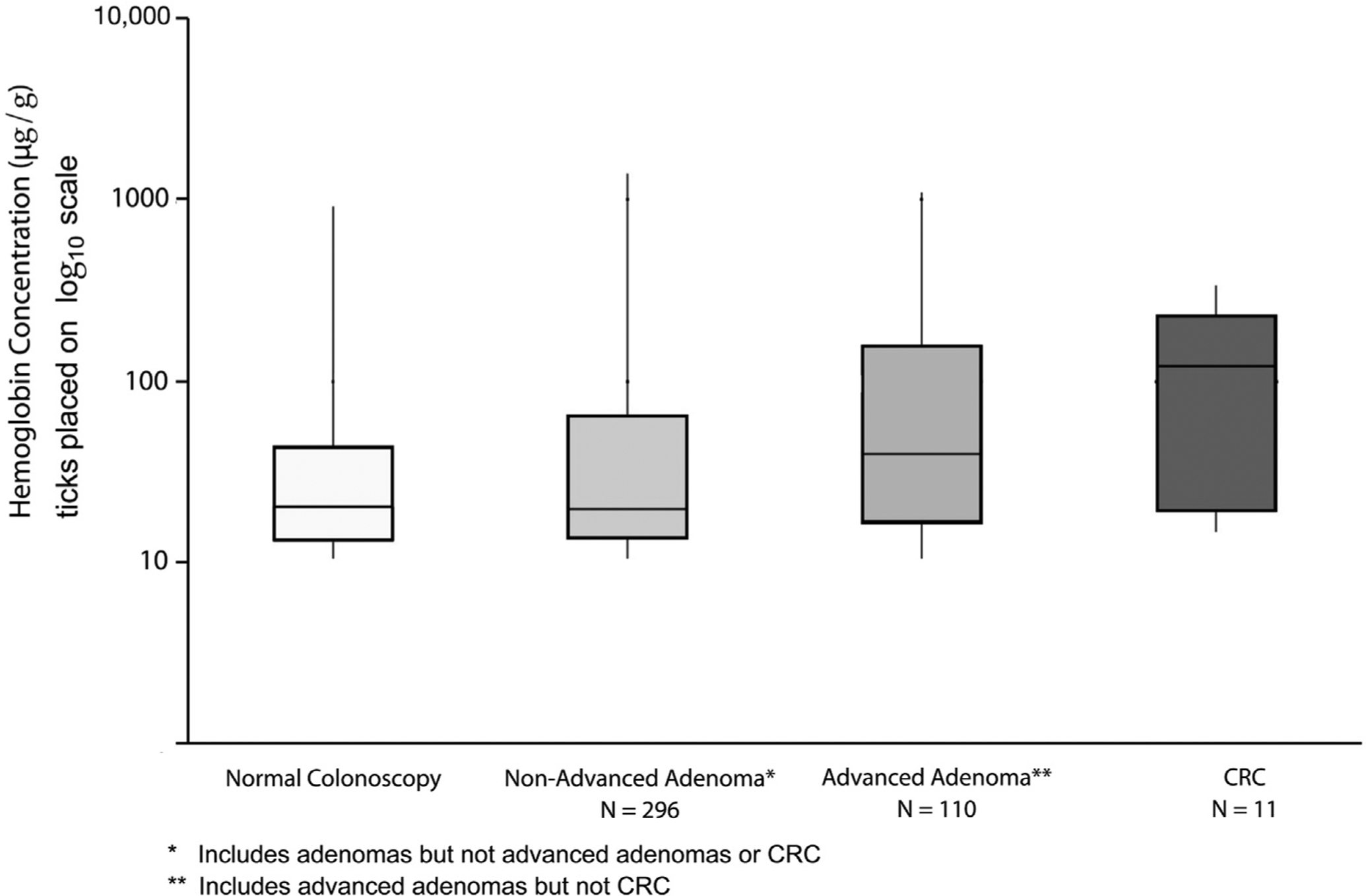
We performed a prospective study of 17,017 uninsured patients, age 50 to 64 years, who were not current with screening and enrolled in a safety-net system in Texas. We reduced the cut-off value for an abnormal FIT result from 20 or more to 10 or more μg hemoglobin/g feces a priori. All patients with abnormal FIT results were offered no-cost diagnostic colonoscopy. We compared proportions of patients with abnormal FIT results and neoplasia yield for standard vs lower cut-off values, as well as absolute hemoglobin concentration distribution among 5838 persons who completed the FIT. Our primary aim was to determine the effects of implementing a lower hemoglobin concentration cut-off value on colonoscopy demand and yield, specifically colorectal cancer (CRC) and advanced neoplasia detection, compared with the standard, higher, hemoglobin concentration cut-off value.
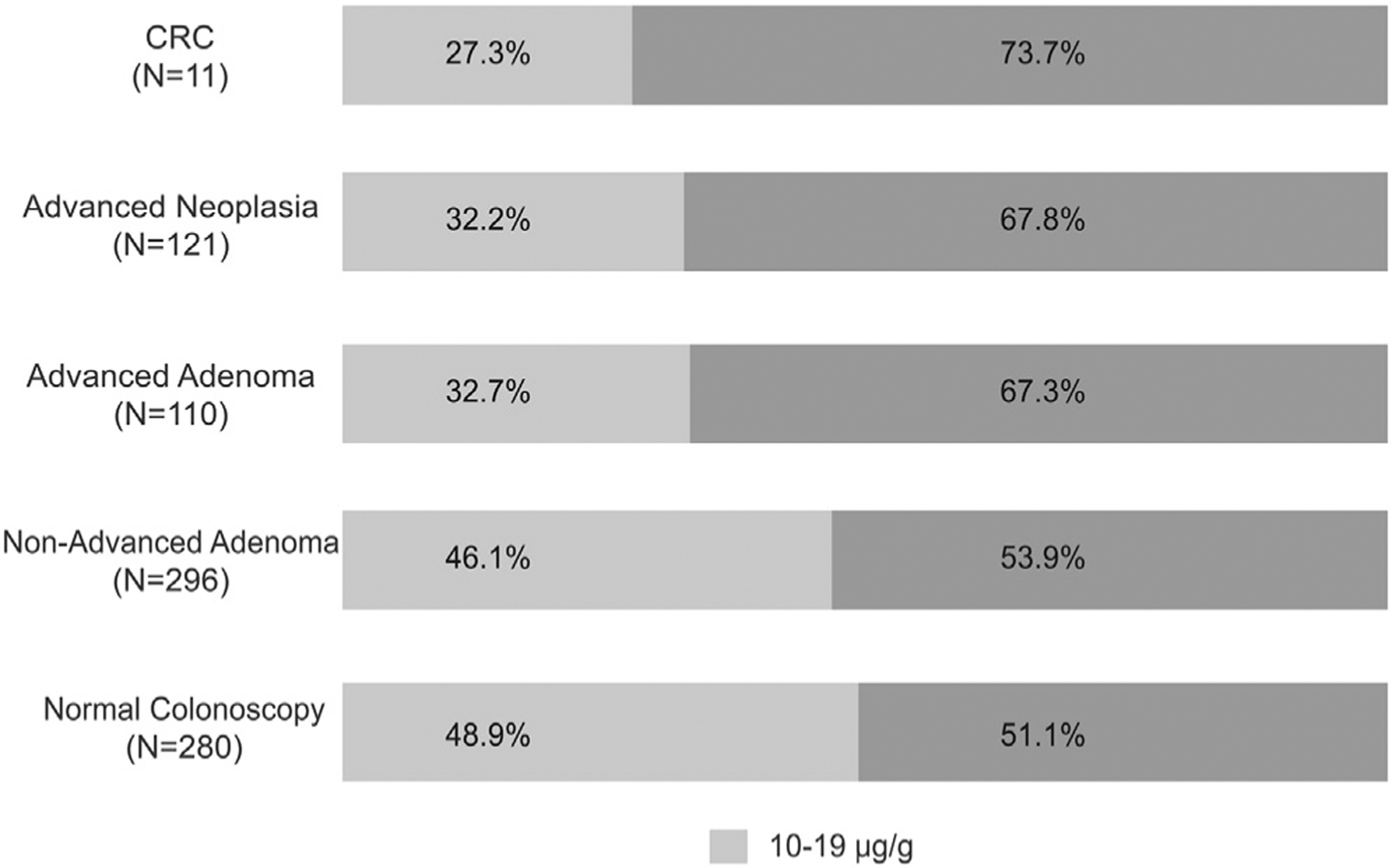
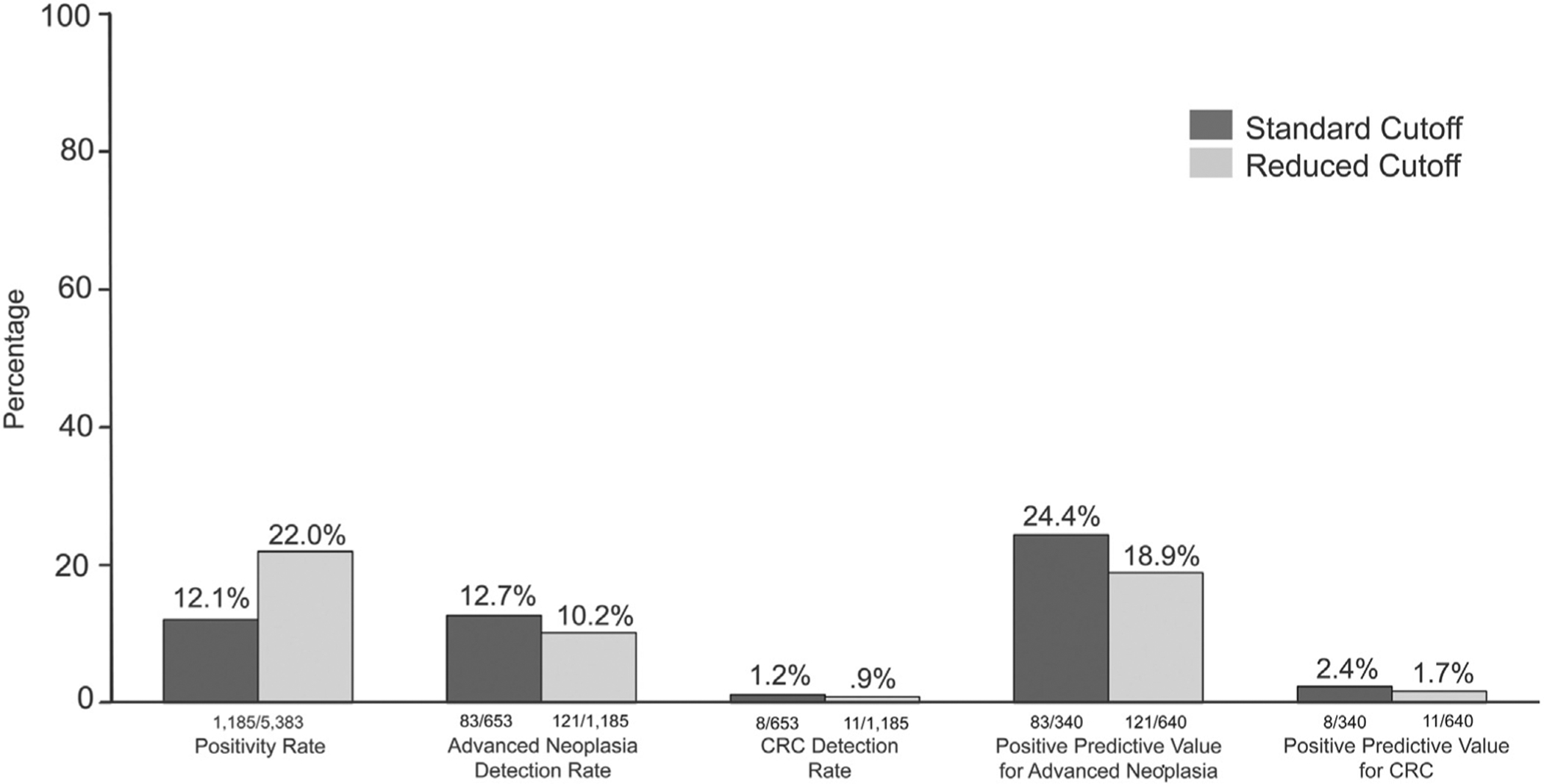
The proportions of patients with abnormal FIT results were 12.3% at the 10 or more μg hemoglobin/g feces and 6.6% at the standard 20 or more μg hemoglobin/g feces cut-off value (P = .0013). Detection rates for the lower vs the standard threshold were 10.2% vs 12.7% for advanced neoplasia (P = .12) and 0.9% vs 1.2% for CRC (P = .718). The positive predictive values were 18.9% for the lower threshold vs 24.4% for the standard threshold for advanced neoplasia (P = .053), and 1.7% vs 2.4% for CRC (P = .659). The number needed to screen to detect 1 case with advanced neoplasia was 45 at the lower threshold compared with 58 at the standard threshold; the number needed to scope to detect 1 case with advanced neoplasia increased from 4 to 5. Most patients with CRC (72.7%) or advanced adenoma (67.3%) had hemoglobin concentrations of 20 or more μg/g feces. In the group with 10 to 19 μg hemoglobin/g feces, there were 3 patients with CRC (3 of 11; 27.3%) and 36 with advanced adenoma (36 of 110; 32.7%) who would not have been detected at the standard positive threshold (advanced neoplasia Pcomparison < .001). The proportion of patients found to have no neoplasia after an abnormal FIT result (false positives) was not significantly higher with the lower cut-off value (44.4%) than the standard cut-off value (39.1%) (P = .1103).
In a prospective study of 17,017 uninsured patients, we found that reducing the abnormal FIT result cut-off value (to ≥10 μg hemoglobin/g feces) might increase detection of advanced neoplasia, but doubled the proportion of patients requiring a diagnostic colonoscopy. If colonoscopy capacity permits, health systems that use quantitative FITs should consider lowering the abnormal cut-off value to optimize CRC detection and prevention. (ClinicalTrials.gov no: NCT01946282.).
结直肠癌筛查中使用的非侵入性检测,如粪便免疫化学检测(FIT),更易被接受,但与结肠镜检查相比,其检测肿瘤的敏感性较低。我们研究了在邮寄外展计划中,降低血红蛋白异常 FIT 结果的截断浓度是否会增加高级别肿瘤的检出率。
我们对 17017 名未参保、年龄在 50 至 64 岁之间、未进行过筛查且参加了德克萨斯州安全网系统的患者进行了前瞻性研究。我们将异常 FIT 结果的截断值从 20μg 或以上降低到 10μg 或以上血红蛋白/粪便。所有异常 FIT 结果的患者都被提供免费的诊断性结肠镜检查。我们比较了标准和较低截断值的异常 FIT 结果和肿瘤检出率,以及完成 FIT 的 5838 人血红蛋白浓度的绝对分布。我们的主要目的是确定实施较低的血红蛋白浓度截断值对结肠镜检查需求和检出率的影响,特别是对结直肠癌(CRC)和高级别肿瘤的检测,与标准、较高的血红蛋白浓度截断值相比。
血红蛋白浓度截断值为 10μg 或以上的患者异常 FIT 结果比例为 12.3%,而标准截断值为 20μg 或以上的患者异常 FIT 结果比例为 6.6%(P=0.0013)。与标准阈值相比,较低阈值的检测率为高级别肿瘤 10.2% vs 12.7%(P=0.12)和 CRC 0.9% vs 1.2%(P=0.718)。较低阈值的阳性预测值为高级别肿瘤 18.9%,而标准阈值为 24.4%(P=0.053),CRC 为 1.7%和 2.4%(P=0.659)。检测 1 例高级别肿瘤所需的筛查人数在较低阈值为 45,而在标准阈值为 58;检测 1 例高级别肿瘤所需的结肠镜检查人数从 4 例增加到 5 例。大多数 CRC(72.7%)或高级腺瘤(67.3%)患者的血红蛋白浓度为 20μg/g 粪便或以上。在血红蛋白浓度为 10 至 19μg/g 粪便的患者中,有 3 例 CRC(3/11;27.3%)和 36 例高级腺瘤(36/110;32.7%)未在标准阳性阈值(高级别肿瘤 P 比较<0.001)中检出。异常 FIT 结果后发现无肿瘤的患者(假阳性)比例(44.4%)与标准截断值(39.1%)相比,并没有显著升高(P=0.1103)。
在一项对 17017 名未参保患者的前瞻性研究中,我们发现降低异常 FIT 结果的截断值(≥10μg 血红蛋白/g 粪便)可能会增加高级别肿瘤的检出率,但会使需要诊断性结肠镜检查的患者比例增加一倍。如果结肠镜检查能力允许,使用定量 FIT 的卫生系统应考虑降低异常截断值,以优化 CRC 的检测和预防。(临床试验编号:NCT01946282.)