Vaccine and Infectious Disease Division, Fred Hutchinson Cancer Research Center, Seattle, Washington.
Division of Infectious Diseases, University of Nebraska Medical Center, Omaha.
Clin Infect Dis. 2020 Mar 17;70(7):1421-1428. doi: 10.1093/cid/ciz409.
Outpatient antibiotic prescribing for acute upper respiratory infections (URIs) is a high-priority target for antimicrobial stewardship that has not been described for cancer patients.
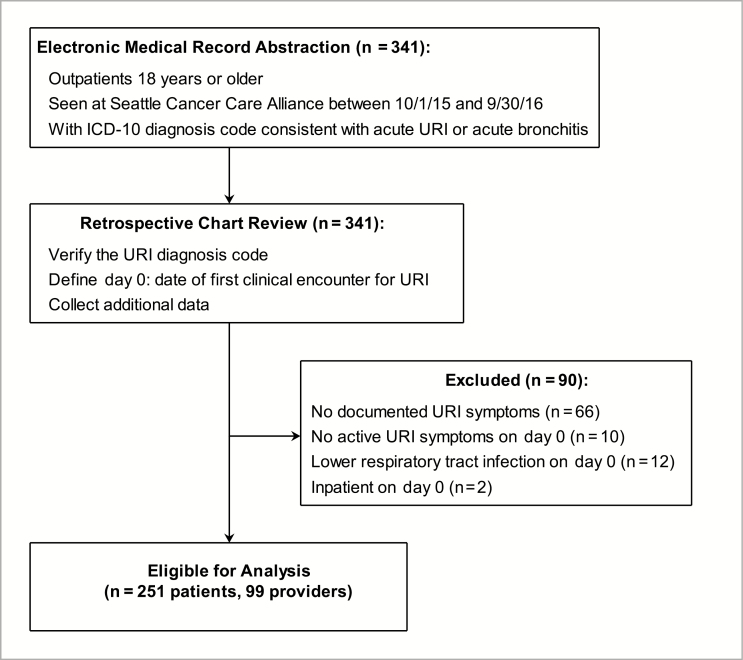
We conducted a retrospective cohort study of adult patients at an ambulatory cancer center with URI diagnoses from 1 October 2015 to 30 September 2016. We obtained antimicrobial prescribing, respiratory viral testing, and other clinical data at first encounter for the URI through day 14. We used generalized estimating equations to test associations of baseline factors with antibiotic prescribing.
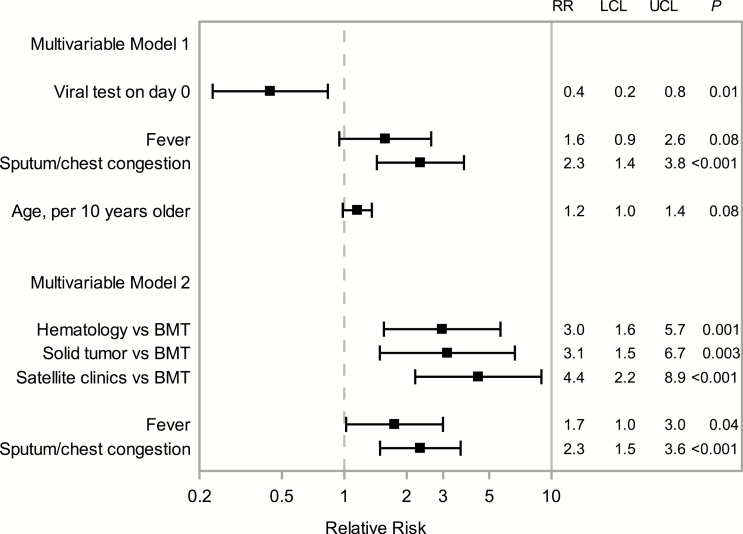
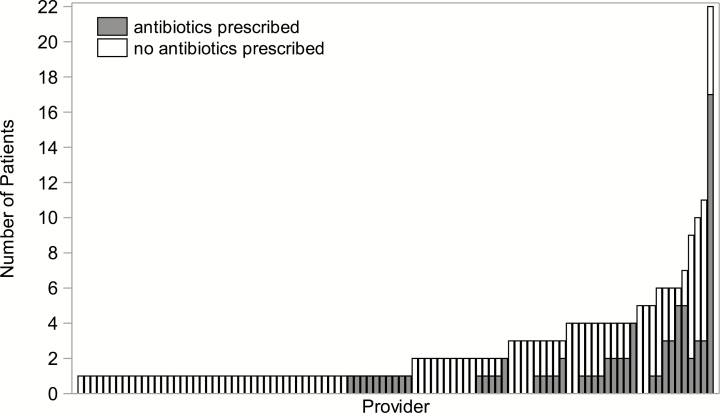
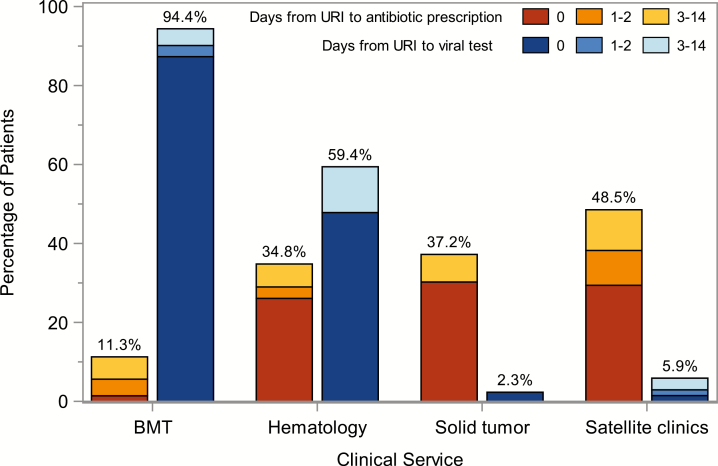
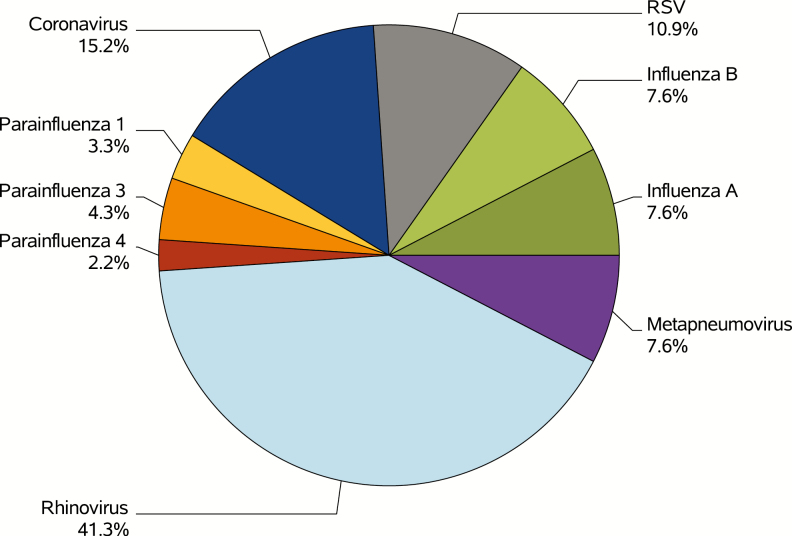
Of 341 charts reviewed, 251 (74%) patients were eligible for analysis. Nearly one-third (32%) of patients were prescribed antibiotics for URIs. Respiratory viruses were detected among 85 (75%) of 113 patients tested. Antibiotic prescribing (P = .001) and viral testing (P < .001) varied by clinical service. Sputum production or chest congestion was associated with higher risk of antibiotic prescribing (relative risk [RR], 2.3; 95% confidence interval [CI], 1.4-3.8; P < .001). Viral testing on day 0 was associated with lower risk of antibiotic prescribing (RR, 0.4; 95% CI 0.2-0.8; P = .01), though collinearity between viral testing and clinical service limited our ability to separate these effects on prescribing.
Nearly one-third of hematology-oncology outpatients were prescribed antibiotics for URIs, despite viral etiologies identified among 75% of those tested. Antibiotic prescribing was significantly lower among patients who received an initial respiratory viral test. The role of viral testing in antibiotic prescribing for URIs in outpatient oncology settings merits further study.
门诊开具急性上呼吸道感染(URIs)抗生素处方是抗菌药物管理的一个高度优先目标,但尚未针对癌症患者进行描述。
我们对 2015 年 10 月 1 日至 2016 年 9 月 30 日期间在一家门诊癌症中心就诊的 URIs 诊断的成年患者进行了回顾性队列研究。我们通过第 14 天获得了 URIs 首次就诊时的抗生素处方、呼吸道病毒检测和其他临床数据。我们使用广义估计方程来检验基线因素与抗生素处方之间的关联。
在审查的 341 份图表中,有 251 份(74%)患者符合分析条件。近三分之一(32%)的患者因 URIs 开具了抗生素。在接受检测的 113 名患者中,有 85 名(75%)检测到呼吸道病毒。抗生素处方(P=.001)和病毒检测(P <.001)因临床科室而异。痰产生或胸部充血与抗生素处方风险增加相关(相对风险 [RR],2.3;95%置信区间 [CI],1.4-3.8;P <.001)。在第 0 天进行病毒检测与抗生素处方风险降低相关(RR,0.4;95%CI 0.2-0.8;P=.01),但病毒检测与临床科室之间的共线性限制了我们分离这些对处方影响的能力。
尽管在接受检测的患者中 75%确定了病毒病因,但仍有近三分之一的血液科-肿瘤科门诊患者因 URIs 开具了抗生素处方。在最初接受呼吸道病毒检测的患者中,抗生素处方明显减少。在门诊肿瘤学环境中,URIs 病毒检测在抗生素处方中的作用值得进一步研究。