Department of Cardiac Surgery, University Hospital Heidelberg, Heidelberg, Germany.
ESC Heart Fail. 2019 Aug;6(4):694-700. doi: 10.1002/ehf2.12447. Epub 2019 May 16.
The occurrence of hyperbilirubinaemia after heart surgery using cardiopulmonary bypass or post-operative heart failure is fairly common. We investigated the incidence, predictive value, and post-operative outcome of hyperbilirubinaemia after cardiac surgery in an effort to identify potential risk factors and significance on clinical outcome.
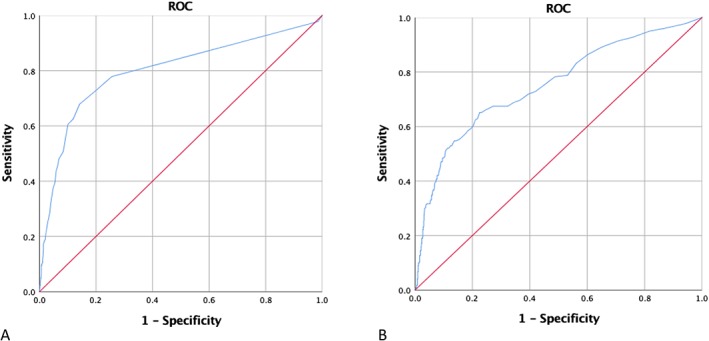
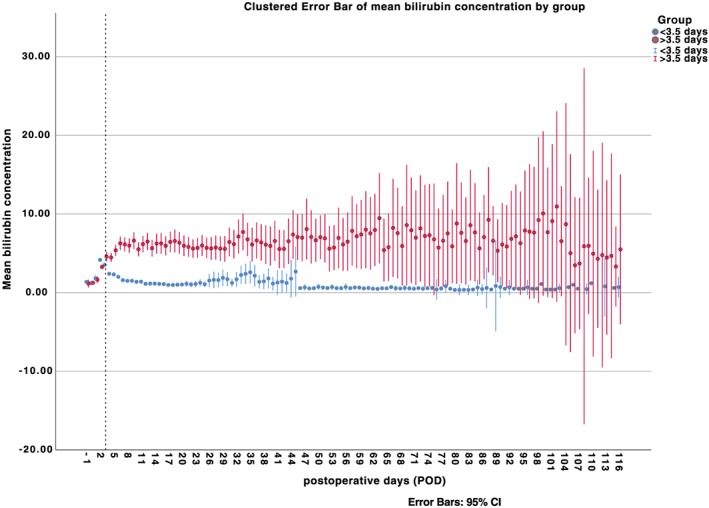
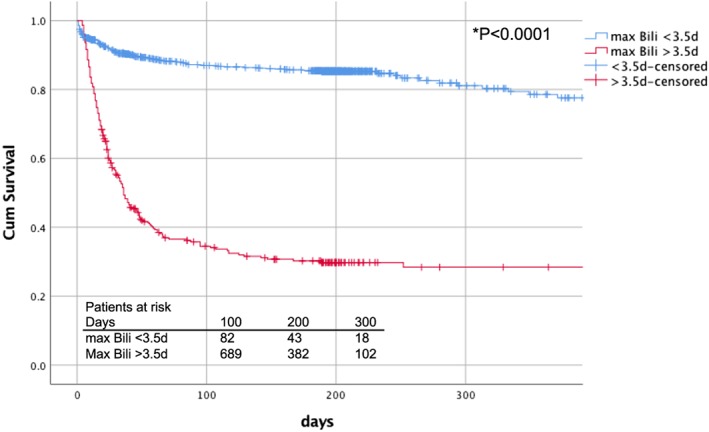
Between 2006 and 2016, 1272 (10.1%) out of 12 556 patients developed hyperbilirubinaemia, defined as bilirubin concentration >3 mg/dL, during post-operative course at our institution. All patients who were operated using cardiopulmonary bypass were included. Hepatic dysfunction was diagnosed preoperatively in 200 patients (15.7%), whereas mean model of end-stage liver disease score was 11.22 ± 4.99. Early mortality was 17.4% with age [hazard ratio (HR) 1.019, 95% confidence interval (CI) 1.008-1.029; P = 0.001], diabetes (HR 1.115, CI 1.020-1.220; P = 0.017), and emergent procedures (HR 1.315, CI 1.012-1.710) as multivariate predictors. Post-operative predictors were low-output syndrome (HR 3.193, 95% CI 2.495-4.086; P < 0.001), blood transfusion (HR 1.0, CI 1.0-1.0; P < 0.001), and time to peak bilirubin (HR 1.1, CI 1.0-1.1; P < 0.001). We found an increased correlation with mortality at 3.5 post-operative day as well as an optimal cut-off value for bilirubin of 5.35 mg/dL. A maximum bilirubin of 25.5 mg/dL was associated with 99% mortality. Survival analysis showed significantly decreased survival for patients who developed late, rather than early, hyperbilirubinaemia.
Post-operative hyperbilirubinaemia is a prevalent threat after cardiopulmonary bypass, associated with high early mortality. The timing and amount of peak bilirubin concentration are linked to the underlying pathology and are predictors of post-operative outcome. Patients with late development of steep hyperbilirubinaemia warrant meticulous post-operative care optimizing cardiac and end organ functions before reaching the point of no return.
体外循环心脏手术后或术后心力衰竭引起的高胆红素血症相当常见。我们研究了心脏手术后高胆红素血症的发生率、预测价值和术后结果,以确定潜在的危险因素和对临床结果的意义。
在我们的机构中,2006 年至 2016 年间,1272 例(10.1%)12556 例患者在术后期间出现高胆红素血症,定义为胆红素浓度>3mg/dL。所有接受体外循环手术的患者均包括在内。术前诊断为肝功能障碍 200 例(15.7%),平均终末期肝病模型评分 11.22±4.99。早期死亡率为 17.4%,年龄[风险比(HR)1.019,95%置信区间(CI)1.008-1.029;P=0.001]、糖尿病(HR 1.115,CI 1.020-1.220;P=0.017)和急诊手术(HR 1.315,CI 1.012-1.710)是多变量预测因子。术后预测因子为低心输出量综合征(HR 3.193,95%CI 2.495-4.086;P<0.001)、输血(HR 1.0,CI 1.0-1.0;P<0.001)和胆红素峰值时间(HR 1.1,CI 1.0-1.1;P<0.001)。我们发现与术后第 3.5 天的死亡率呈正相关,胆红素的最佳截断值为 5.35mg/dL。胆红素最大值为 25.5mg/dL,死亡率为 99%。生存分析显示,迟发性高胆红素血症患者的生存时间明显缩短,而非早发性高胆红素血症患者。
体外循环后高胆红素血症是体外循环后普遍存在的威胁,与早期高死亡率相关。胆红素峰值浓度的时间和量与潜在的病理有关,是术后结果的预测因子。发生急剧高胆红素血症的患者需要在到达不可逆转的点之前进行精心的术后护理,以优化心脏和终末器官的功能。