Department of Radiation Oncology, Gunma University Graduate School of Medicine, Showa-machi, Maebashi, Gunma, Japan.
Department of Radiation Oncology, Saitama Medical University International Medical Center, 1397-1 Yamane, Hidaka, Saitama, Japan.
J Radiat Res. 2019 Jul 1;60(4):490-500. doi: 10.1093/jrr/rrz023.
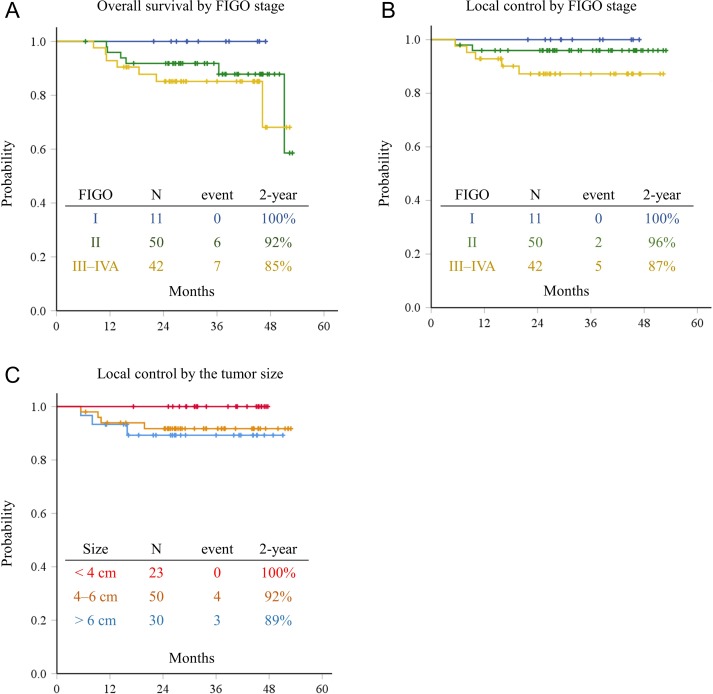
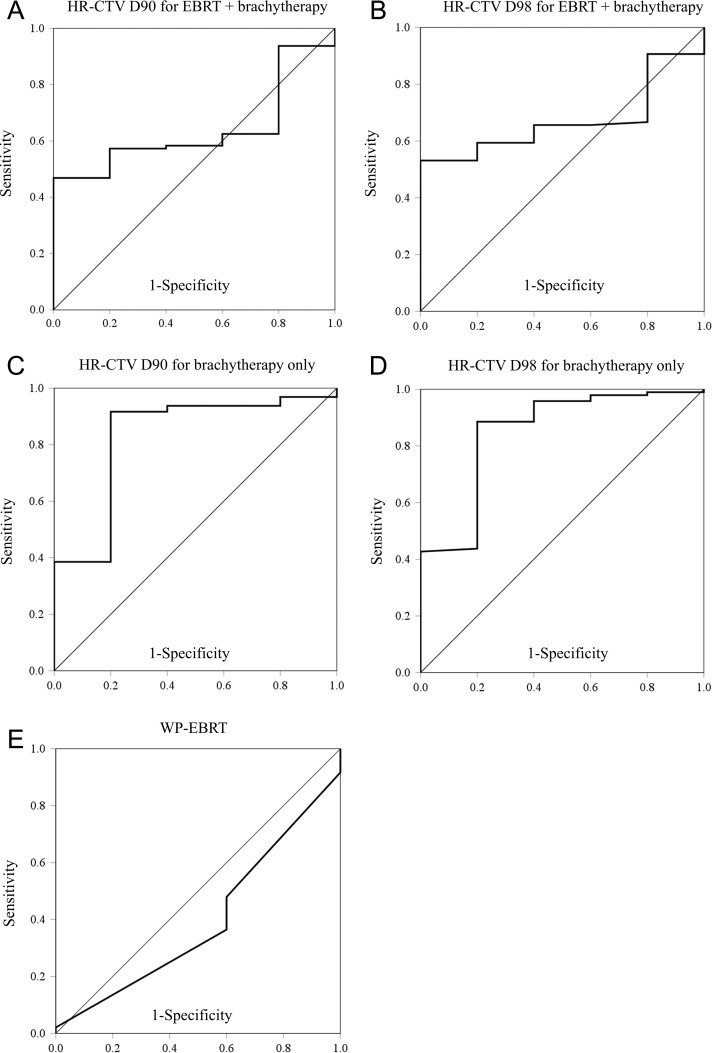
Definitive radiotherapy for cervical cancer consists of external-beam radiotherapy (EBRT) and brachytherapy. In EBRT, a central shield (CS) reduces the dose to the rectum and bladder. The combination of whole-pelvic (WP)- and CS-EBRT and brachytherapy is the standard radiotherapy protocol in Japan. Despite clinical studies, including multi-institutional clinical trials, showing that the Japanese treatment protocol yields favorable treatment outcomes with low rates of late radiation toxicities, dose-volume parameters for the Japanese treatment protocol remain to be established. We conducted a retrospective dose-volume analysis of 103 patients with uterine cervical cancer treated with the Japanese protocol using computed tomography-based adaptive brachytherapy. The 2-year overall survival and 2-year local control rates according to FIGO stage were 100% and 100% for Stage I, 92% and 94% for Stage II, and 85% and 87% for Stage III-IV, respectively. Late adverse effects in the rectum and bladder were acceptable. Receiver operating characteristic analysis discriminated recurrence within the high-risk clinical target volume (HR-CTV) (n = 5) from no local recurrence (n = 96), with the optimal response obtained at a dose of 36.0 GyEQD2 for HR-CTV D90 and 28.0 GyEQD2 for HR-CTV D98. These values were used as cut-offs in Fisher exact tests to show that high HR-CTV D90 and HR-CTV D98 doses for brachytherapy sessions were significantly associated with tumor control within the HR-CTV. These data suggest a contribution of brachytherapy to local tumor control in WP- and CS-EBRT and brachytherapy combination treatment, warranting validation in multi-institutional prospective studies.
根治性宫颈癌放疗包括外照射放疗(EBRT)和近距离放疗。在 EBRT 中,中央屏蔽(CS)可降低直肠和膀胱的剂量。全盆腔(WP)-CS-EBRT 和近距离放疗的联合是日本的标准放疗方案。尽管包括多机构临床试验在内的临床研究表明,日本的治疗方案具有良好的治疗效果且晚期放射毒性发生率低,但日本治疗方案的剂量-体积参数仍有待确定。我们使用基于 CT 的自适应近距离放疗对 103 例接受日本方案治疗的宫颈癌患者进行了回顾性剂量-体积分析。根据 FIGO 分期,2 年总生存率和 2 年局部控制率分别为 I 期 100%和 100%,II 期 92%和 94%,III-IV 期 85%和 87%。直肠和膀胱的晚期不良反应是可以接受的。ROC 分析区分了高危临床靶区(HR-CTV)内的复发(n = 5)和无局部复发(n = 96),HR-CTV D90 的最佳反应剂量为 36.0 GyEQD2,HR-CTV D98 的最佳反应剂量为 28.0 GyEQD2。这些值被用作 Fisher 精确检验的截止值,表明近距离放疗过程中 HR-CTV D90 和 HR-CTV D98 剂量较高与 HR-CTV 内肿瘤控制显著相关。这些数据表明,近距离放疗对 WP-CS-EBRT 和近距离放疗联合治疗中的局部肿瘤控制有一定贡献,值得在多机构前瞻性研究中进一步验证。