Department of Radiation Oncology, Osaka University Graduate School of Medicine, 2-2 (D10) Yamada-oka, Suita, Osaka 565-0871, Japan.
Department of Radiology, Kaizuka city hospital, 3-10-20 Hori, Kaizuka, Osaka, 597-0015, Japan.
J Radiat Res. 2021 May 12;62(3):502-510. doi: 10.1093/jrr/rraa138.
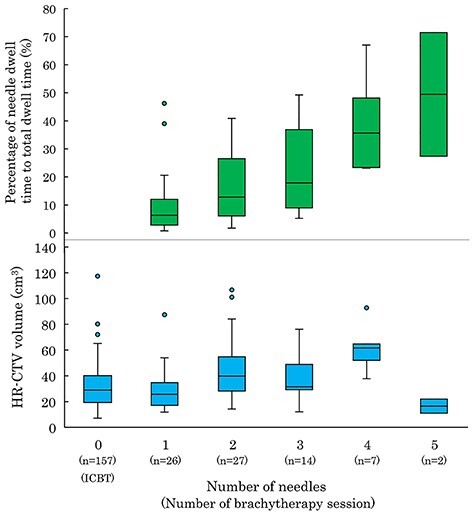
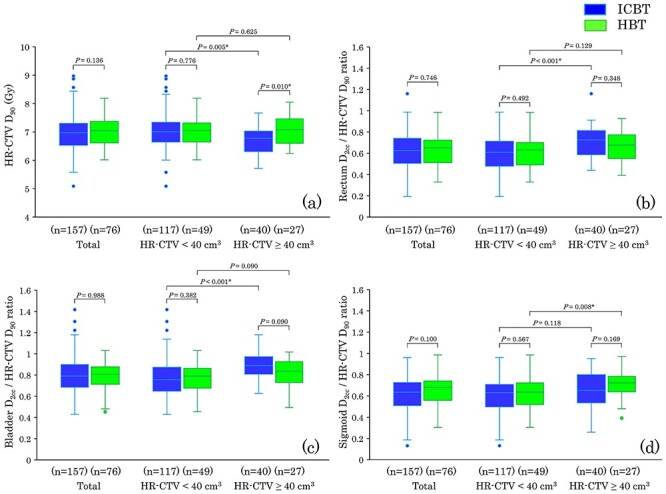
The aim of this study was to assess the feasibility of planning dose-volume histogram (DVH) parameters in computed tomography-based 3D image-guided brachytherapy for locally advanced cervical cancer. In a prospective multi-institutional study, 60 patients with stage IIA2-IVA cervical cancer from eight institutions were treated with external beam radiotherapy using central shielding and intracavitary or hybrid (combined intracavitary/interstitial) brachytherapy (HBT). The dose constraints were set as a cumulative linear quadratic equivalent dose (EQD2) of at least 60 Gy for high-risk clinical target volume (HR-CTV) D90, D2cc ≤ 75 Gy for rectum, D2cc ≤ 90 Gy for bladder and D2cc ≤ 75 Gy for sigmoid. The median HR-CTV D90 was 70.0 Gy (range, 62.8-83.7 Gy) in EQD2. The median D2cc of rectum, bladder and sigmoid was 57.1 Gy (range, 39.8-72.1 Gy), 68.9 Gy (range, 46.5-84.9 Gy) and 57.2 Gy (range, 39.2-71.2 Gy) in EQD2, respectively. In 76 of 233 sessions (33%), 23 patients underwent HBT, and the median number of interstitial needles was 2 (range, 1-5). HBT for a bulky HR-CTV (≥40 cm3) significantly improved the HR-CTV D90 compared with intracavitary brachytherapy alone (P = 0.010). All patients fulfilled the dose constrains for target and at risk organs by undergoing HBT in one-third of sessions. We conclude that the planning DVH parameters used in our protocol are clinically feasible.
本研究旨在评估在基于 CT 的 3D 图像引导近距离放疗中规划剂量体积直方图 (DVH) 参数治疗局部晚期宫颈癌的可行性。在一项前瞻性多中心研究中,来自 8 个机构的 60 例 IIA2-IVA 期宫颈癌患者接受了外部束放疗,采用中央屏蔽和腔内或混合(腔内/间质联合)近距离放疗 (HBT)。剂量限制设定为高危临床靶区 (HR-CTV) D90 的累积线性二次等效剂量 (EQD2) 至少 60Gy,直肠 D2cc ≤ 75Gy,膀胱 D2cc ≤ 90Gy 和乙状结肠 D2cc ≤ 75Gy。中位 HR-CTV D90 的 EQD2 为 70.0Gy(范围,62.8-83.7Gy)。直肠、膀胱和乙状结肠的中位 D2cc 分别为 57.1Gy(范围,39.8-72.1Gy)、68.9Gy(范围,46.5-84.9Gy)和 57.2Gy(范围,39.2-71.2Gy)。在 233 次治疗中,有 76 次(33%)采用了 HBT,其中 23 例患者接受了 HBT,间质针的中位数为 2 根(范围,1-5 根)。与单纯腔内近距离放疗相比,对于大体积 HR-CTV(≥40cm3),HBT 显著提高了 HR-CTV D90(P=0.010)。通过 HBT 进行三分之一的治疗,所有患者均满足靶区和危险器官的剂量限制。我们的结论是,我们方案中使用的计划 DVH 参数在临床上是可行的。