The George Institute for Global Health, University of Oxford, Oxford, United Kingdom.
Nuffield Department of Orthopaedics, Rheumatology and Musculoskeletal Sciences, Nuffield Orthopaedic Centre, University of Oxford, Oxford, United Kingdom.
PLoS Med. 2019 May 21;16(5):e1002805. doi: 10.1371/journal.pmed.1002805. eCollection 2019 May.
Effective management of heart failure is complex, and ensuring evidence-based practice presents a major challenge to health services worldwide. Over the past decade, the United Kingdom introduced a series of national initiatives to improve evidence-based heart failure management, including a landmark pay-for-performance scheme in primary care and a national audit in secondary care started in 2004 and 2007, respectively. Quality improvement efforts have been evaluated within individual clinical settings, but patterns of care across its continuum, although a critical component of chronic disease management, have not been studied. We have designed this study to investigate patients' trajectories of care around the time of diagnosis and their variation over time by age, sex, and socioeconomic status.
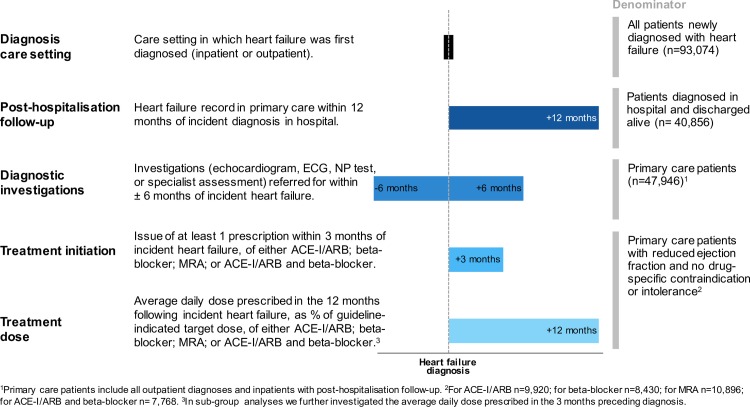
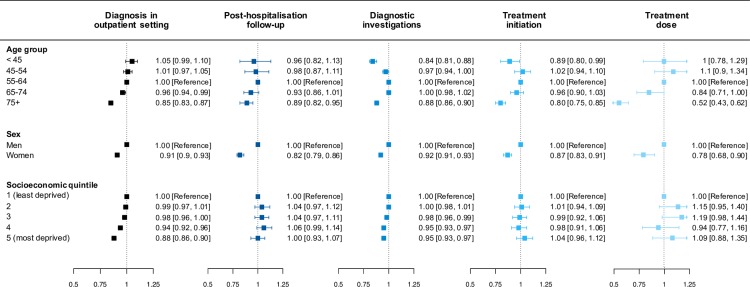
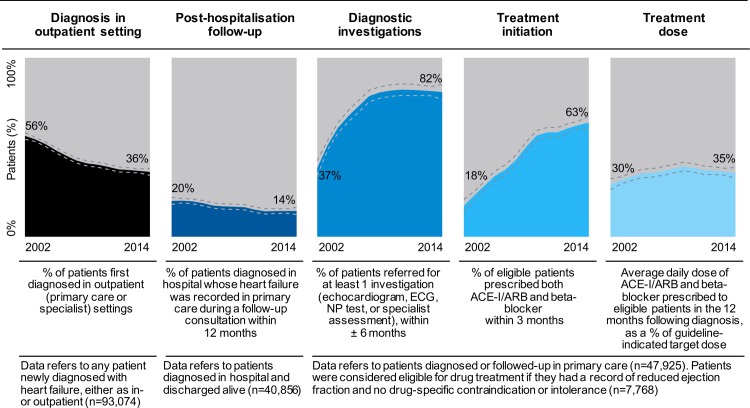
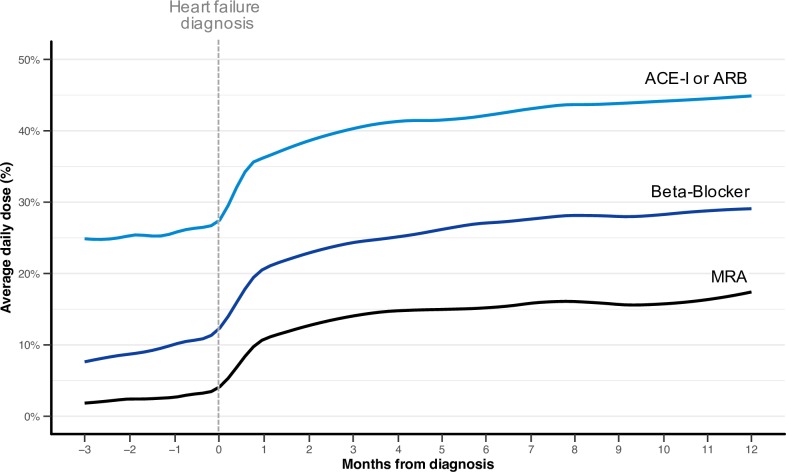
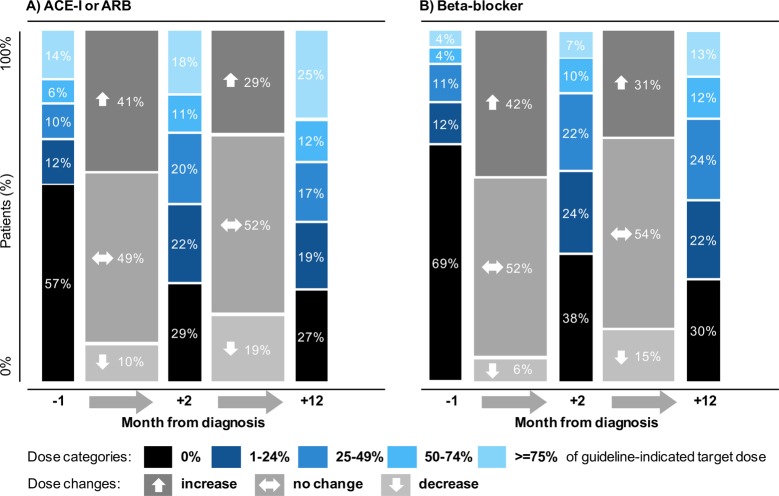
For this retrospective population-based study, we used linked primary and secondary health records from a representative sample of the UK population provided by the Clinical Practice Research Datalink (CPRD). We identified 93,074 individuals newly diagnosed with heart failure between 2002 and 2014, with a mean age of 76.7 years and of which 49% were women. We examined five indicators of care: (i) diagnosis care setting (inpatient or outpatient), (ii) posthospitalisation follow-up in primary care, (iii) diagnostic investigations, (iv) prescription of essential drugs, and (v) drug treatment dose. We used Poisson and linear regression models to calculate category-specific risk ratios (RRs) or adjusted differences and 95% confidence intervals (CIs), adjusting for year of diagnosis, age, sex, region, and socioeconomic status. From 2002 to 2014, indicators of care presented diverging trends. Outpatient diagnoses and follow-up after hospital discharge in primary care declined substantially (ranging from 56% in 2002 to 36% in 2014, RR 0.64 [0.62, 0.67] and 20% to 14%, RR 0.73 [0.65, 0.82], respectively). Primary care referral for diagnostic investigations and appropriate initiation of beta blockers and angiotensin-converting-enzyme inhibitors (ACE-Is) or angiotensin receptor blockers (ARBs) both increased significantly (37% versus 82%, RR 2.24 [2.15, 2.34] and 18% versus 63%, RR 3.48 [2.72, 4.43], respectively). Yet, the average daily dose prescribed remained below guideline recommendations (42% for ACE-Is or ARBs, 29% for beta blockers in 2014) and was largely unchanged beyond the first 30 days after diagnosis. Despite increasing rates of treatment initiation, the overall dose prescribed to patients in the 12 months following diagnosis improved little over the period of study (adjusted difference for the combined dose of beta blocker and ACE-I or ARB: +6% [+2%, +10%]). Women and patients aged over 75 years presented significant gaps across all five indicators of care. Our study was limited by the available clinical information, which did not include exact left ventricular ejection fraction values, investigations performed during hospital admissions, or information about follow-up in community heart failure clinics.
Management of heart failure patients in the UK presents important shortcomings that affect screening, continuity of care, and medication titration and disproportionally impact women and older people. National reporting and incentive schemes confined to individual clinical settings have been insufficient to identify these gaps and address patients' long-term care needs.
心力衰竭的有效管理非常复杂,确保循证实践对全球卫生服务提出了重大挑战。在过去的十年中,英国推出了一系列旨在改善基于证据的心力衰竭管理的国家举措,包括初级保健中的一项具有里程碑意义的按绩效付费计划和 2004 年和 2007 年分别在二级保健中启动的国家审计。已经在单个临床环境中评估了质量改进工作,但疾病管理连续性的护理模式,尽管是慢性病管理的重要组成部分,但尚未研究。我们设计了这项研究,以调查患者在诊断时的护理轨迹及其随时间的变化,包括年龄、性别和社会经济地位。
在这项基于人群的回顾性研究中,我们使用了英国代表性人群的初级保健和二级保健记录的链接,这些记录由临床实践研究数据链接(CPRD)提供。我们确定了 2002 年至 2014 年间新诊断为心力衰竭的 93074 名患者,平均年龄为 76.7 岁,其中 49%为女性。我们检查了护理的五个指标:(i)诊断护理环境(住院或门诊),(ii)出院后在初级保健中的随访,(iii)诊断性检查,(iv)开处方的基本药物,和(v)药物治疗剂量。我们使用泊松和线性回归模型计算了特定类别的风险比(RR)或调整后的差异和 95%置信区间(CI),调整了诊断年份、年龄、性别、地区和社会经济地位。从 2002 年到 2014 年,护理指标呈现出不同的趋势。门诊诊断和出院后在初级保健中的随访显著下降(分别从 2002 年的 56%下降到 2014 年的 36%,RR 0.64 [0.62, 0.67]和 20%下降到 14%,RR 0.73 [0.65, 0.82])。初级保健转介进行诊断性检查以及适当开始使用β受体阻滞剂和血管紧张素转换酶抑制剂(ACE-Is)或血管紧张素受体阻滞剂(ARBs)均显著增加(分别从 37%增加到 82%,RR 2.24 [2.15, 2.34]和从 18%增加到 63%,RR 3.48 [2.72, 4.43])。然而,处方的平均日剂量仍低于指南建议(2014 年 ACE-Is 或 ARBs 为 42%,β受体阻滞剂为 29%),并且在诊断后 30 天之后基本不变。尽管治疗开始率增加,但在诊断后 12 个月内,患者的总体剂量处方改善不大(β受体阻滞剂和 ACE-I 或 ARB 联合剂量的调整差异:+6% [+2%,+10%])。女性和 75 岁以上的患者在所有五个护理指标方面都存在显著差距。我们的研究受到现有临床信息的限制,这些信息不包括确切的左心室射血分数值、住院期间进行的检查或社区心力衰竭诊所的随访信息。
英国心力衰竭患者的管理存在重要缺陷,影响了筛查、护理连续性和药物滴定,并且不成比例地影响了女性和老年人。仅局限于单个临床环境的国家报告和激励计划不足以发现这些差距并满足患者的长期护理需求。