Walker Simon, Spackman Eldon, Conrad Nathalie, Emdin Connor A, Griffin Ed, Rahimi Kazem, Sculpher Mark
Centre for Health Economics, University of York, York, UK.
Institute of Public Health, University of Calgary, Calgary, Alberta, Canada.
Open Heart. 2017 Dec 22;4(2):e000726. doi: 10.1136/openhrt-2017-000726. eCollection 2017.
Many patients with heart failure (HF) do not receive recommended treatments, resulting in suboptimal outcomes. We aimed to investigate the impact of implementing recommended HF therapies on health outcomes, and the costs and effectiveness of interventions for improving adherence.
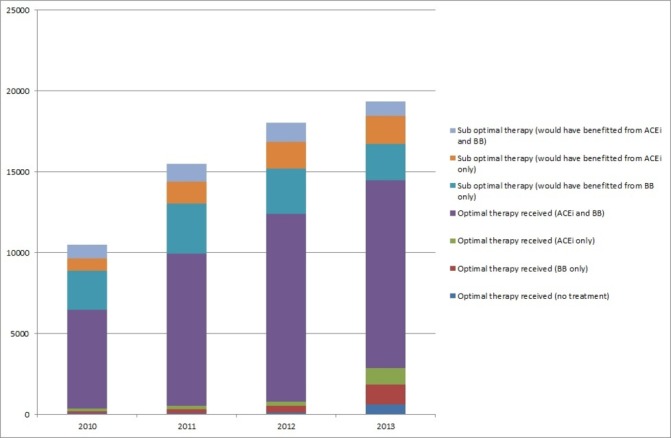
The health benefits of ACE inhibitor (ACEi), beta blockers and optimal therapy (ACEi and beta blockers if not contraindicated) following hospitalisation for HF were combined with evidence on uptake. The aim was to examine how much health was lost as a result of failure to follow guidelines, and how much could be gained using strategies to promote uptake.The net health benefits of different treatments (measured in quality-adjusted life-years (QALY)) were estimated using a decision-analytic model and treatment effectiveness from the literature. Data on the number of patients who would have benefitted from the additional treatments were estimated from 2010 to 2013 using the National Heart Failure Audit.
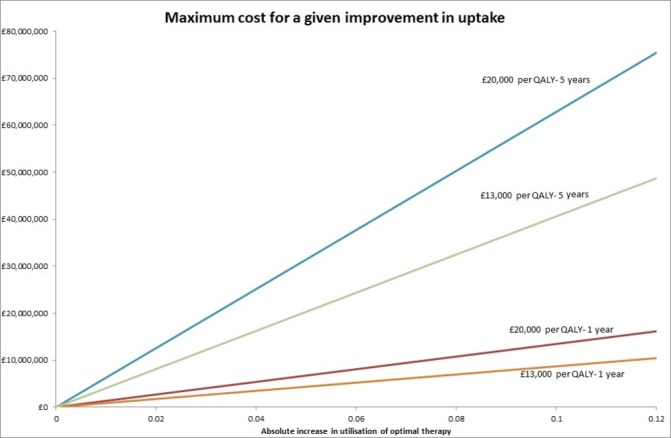
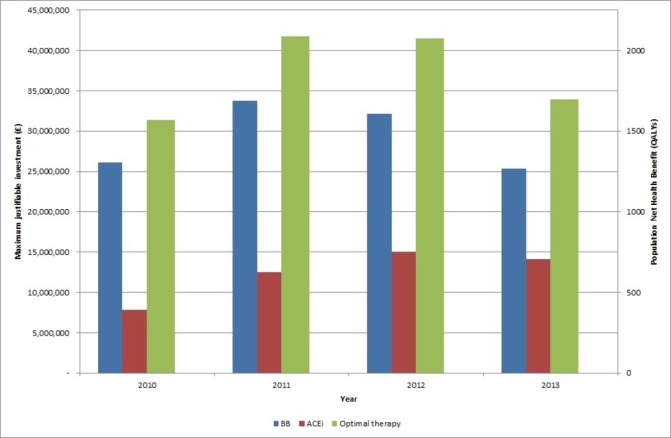
Each recommended treatment was associated with positive net health benefit. In 2010, up to 4019 (38.3%) patients would have benefitted from additional treatments rising to 4886 patients in 2013 (although falling to 25.2% of patients). Failure to follow guidelines resulted in large health losses. In 2010, if all patients had received optimal therapy, 1569 QALYs would have been gained, implying a maximum justifiable investment in interventions to promote uptake of £31.4 million.
Current gaps in translation of evidence to practise in hospitals are associated with significant health losses. Strategies to encourage uptake of guidelines could be effective and cost-effective.
许多心力衰竭(HF)患者未接受推荐治疗,导致治疗效果欠佳。我们旨在研究实施推荐的HF治疗对健康结局的影响,以及改善依从性干预措施的成本和效果。
将HF住院后使用血管紧张素转换酶抑制剂(ACEi)、β受体阻滞剂及最佳治疗(若无禁忌证则使用ACEi和β受体阻滞剂)的健康益处与治疗接受情况的证据相结合。目的是研究因未遵循指南而损失了多少健康,以及使用促进治疗接受的策略可获得多少健康收益。使用决策分析模型和文献中的治疗效果估计不同治疗的净健康益处(以质量调整生命年(QALY)衡量)。利用国家心力衰竭审计数据估计了2010年至2013年期间可能从额外治疗中获益的患者数量。
每种推荐治疗均与正向净健康益处相关。2010年,多达4019名(38.3%)患者可从额外治疗中获益,到2013年这一数字增至4886名患者(尽管占患者总数的比例降至25.2%)。未遵循指南导致大量健康损失。2010年,如果所有患者均接受最佳治疗,将可获得1569个QALY,这意味着促进治疗接受的干预措施的最大合理投资为3140万英镑。
目前医院中证据转化为实践方面的差距与重大健康损失相关。鼓励遵循指南的策略可能有效且具有成本效益。