Güell Estel, Martín-Fernandez Marta, De la Torre Mari C, Palomera Elisabet, Serra Mateu, Martinez Rafael, Solsona Manel, Miró Gloria, Vallès Jordi, Fernández Samuel, Cortés Edgar, Ferrer Vanessa, Morales Marc, Yébenes Juan C, Almirall Jordi, Bermejo-Martin Jesús F
Department of Intensive Care Medicine, Hospital de Mataró, Universitat Autònoma de Barcelona, 08304 Barcelona, Spain.
Grup d'Estudi al Maresme de la Pneumònia Adquirida a la Comunitat (GEMPAC) acreditat per la AGAUR (expedient 2014 SGR 1018), Consorci Sanitari del Maresme, 08204 Mataró, Spain.
J Clin Med. 2019 May 27;8(5):754. doi: 10.3390/jcm8050754.
Community-acquired pneumonia (CAP) is a frequent cause of death worldwide. As recently described, CAP shows different biological endotypes. Improving characterization of these endotypes is needed to optimize individualized treatment of this disease. The potential value of the leukogram to assist prognosis in severe CAP has not been previously addressed.
A cohort of 710 patients with CAP admitted to the intensive care units (ICUs) at Hospital of Mataró and Parc Taulí Hospital of Sabadell was retrospectively analyzed. Patients were split in those with septic shock ( = 304) and those with no septic shock ( = 406). A single blood sample was drawn from all the patients at the time of admission to the emergency room. ICU mortality was the main outcome.
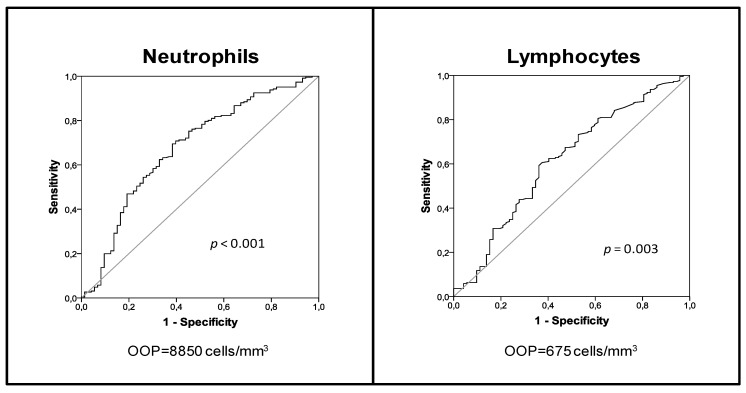
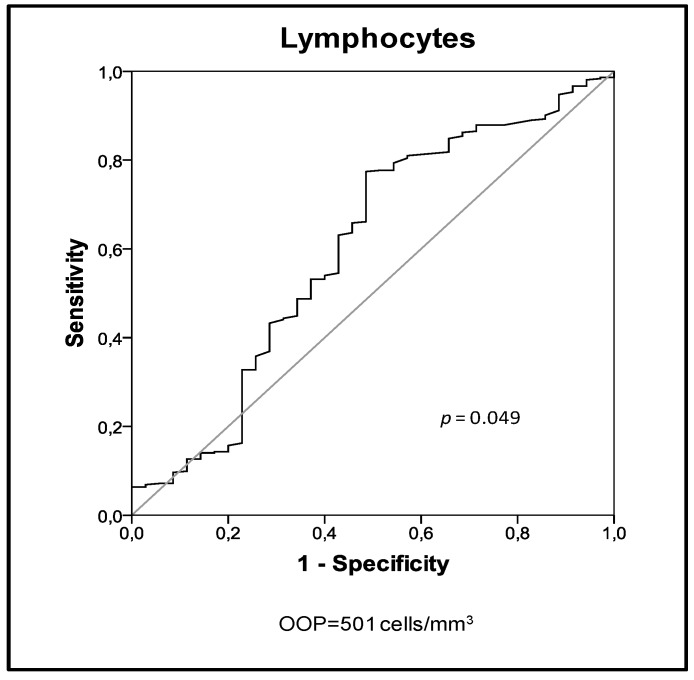
Multivariate analysis demonstrated that lymphopenia <675 cells/mm or <501 cells/mm translated into 2.32- and 3.76-fold risk of mortality in patients with or without septic shock, respectively. In turn, neutrophil counts were associated with prognosis just in the group of patients with septic shock, where neutrophils <8850 cells/mm translated into 3.6-fold risk of mortality.
lymphopenia is a preserved risk factor for mortality across the different clinical presentations of severe CAP (sCAP), while failing to expand circulating neutrophils counts beyond the upper limit of normality represents an incremental immunological failure observed just in those patients with the most severe form of CAP, septic shock.
社区获得性肺炎(CAP)是全球范围内常见的死亡原因。如最近所描述的,CAP表现出不同的生物学亚型。为优化该疾病的个体化治疗,需要更好地对这些亚型进行特征描述。白细胞计数在重症CAP预后评估中的潜在价值此前尚未得到探讨。
对马塔罗医院和萨瓦德尔陶利公园医院重症监护病房(ICU)收治的710例CAP患者进行回顾性分析。患者分为发生感染性休克的患者(n = 304)和未发生感染性休克的患者(n = 406)。所有患者在急诊室入院时采集一份血样。ICU死亡率是主要观察指标。
多因素分析表明,淋巴细胞减少<675个细胞/mm³或<501个细胞/mm³分别使发生或未发生感染性休克的患者死亡风险增加2.32倍和3.76倍。反过来,中性粒细胞计数仅在感染性休克患者组中与预后相关,其中中性粒细胞<8850个细胞/mm³使死亡风险增加3.6倍。
淋巴细胞减少是重症CAP(sCAP)不同临床表现类型中持续存在的死亡危险因素,而未能使循环中性粒细胞计数超过正常上限代表仅在最严重形式的CAP即感染性休克患者中观察到的免疫功能进一步衰竭。