Department of Oncology, Wayne State University School of Medicine, Detroit, MI, USA.
Population Studies and Disparities Research Program, Karmanos Cancer Institute, Detroit, MI, USA.
J Cancer Surviv. 2019 Jun;13(3):429-437. doi: 10.1007/s11764-019-00764-y. Epub 2019 May 29.
Estimate prevalence of types of cancer-related financial hardship by race and test whether they are associated with limiting care due to cost.
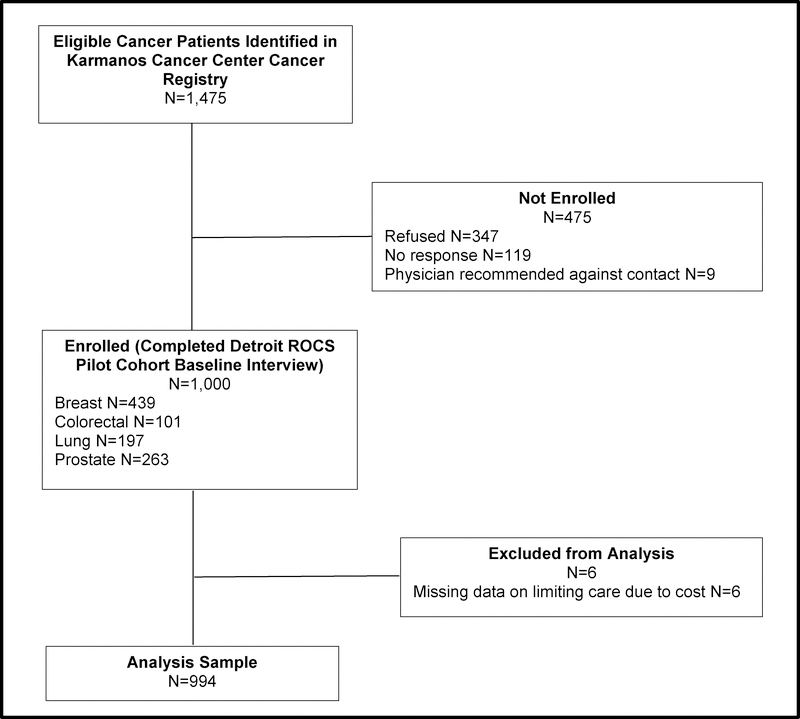
We used data from 994 participants (411 white, 583 African American) in a hospital-based cohort study of survivors diagnosed with breast, colorectal, lung, or prostate cancer since January 1, 2013. Financial hardship included decreased income, borrowing money, cancer-related debt, and accessing assets to pay for cancer care. Limiting care included skipping doses of prescribed medication, refusing treatment, or not seeing a doctor when needed due to cost. Logistic regression models controlled for sociodemographic factors.
More African American than white survivors reported financial hardship (50.3% vs. 41.0%, p = 0.005) and limiting care (20.0% vs. 14.2%, p = 0.019). More white than African American survivors reported utilizing assets (9.3% vs. 4.8%, p = 0.006), while more African American survivors reported cancer-related debt (30.5% vs. 18.5%, p < 0.001). Survivors who experienced financial hardship were 4.4 (95% CI: 2.9, 6.6) times as likely to limit care as those who did not. Borrowing money, cancer-related debt, and decreased income were each independently associated with limiting care, while accessing assets was not.
The prevalence of some forms of financial hardship differed by race, and these were differentially associated with limiting care due to cost.
The ability to use assets to pay for cancer care may protect survivors from limiting care due to cost. This has differential impacts on white and African American survivors.
按种族估计癌症相关经济困难的类型的患病率,并检验这些困难是否与因费用而限制治疗相关。
我们使用了 994 名(411 名白人,583 名非裔美国人)参与者的数据,这些参与者是在 2013 年 1 月 1 日以来被诊断出患有乳腺癌、结直肠癌、肺癌或前列腺癌的医院队列研究中的幸存者。经济困难包括收入减少、借款、与癌症相关的债务以及动用资产来支付癌症治疗费用。限制治疗包括减少规定药物的剂量、拒绝治疗或因费用而在需要时不去看医生。逻辑回归模型控制了社会人口统计学因素。
与白人幸存者相比,更多的非裔美国幸存者报告了经济困难(50.3%对 41.0%,p=0.005)和限制治疗(20.0%对 14.2%,p=0.019)。与非裔美国幸存者相比,更多的白人幸存者报告了动用资产(9.3%对 4.8%,p=0.006),而更多的非裔美国幸存者报告了与癌症相关的债务(30.5%对 18.5%,p<0.001)。经历经济困难的幸存者限制治疗的可能性是未经历经济困难的幸存者的 4.4 倍(95%CI:2.9,6.6)。借款、与癌症相关的债务和收入减少均与限制治疗独立相关,而动用资产则没有。
某些形式的经济困难的患病率因种族而异,而这些困难与因费用而限制治疗有不同的关联。
使用资产支付癌症治疗费用的能力可能会保护幸存者免受因费用而限制治疗。这对白人幸存者和非裔美国幸存者有不同的影响。