Department of Surgery, Central Hospital of Kristianstad, SE-291 85, Kristianstad, Sweden.
Department of Clinical Sciences Malmö, Lund University, Malmö, Sweden.
BMC Cancer. 2019 Jun 25;19(1):626. doi: 10.1186/s12885-019-5823-x.
Sentinel node biopsy (SNB) is the standard procedure for axillary staging in patients with clinically lymph node negative invasive breast cancer. Completion axillary lymph node dissection (c-ALND) may not be necessary for all patients as a significant number of patients have no further metastases in non-sentinel nodes (non-SN) and c-ALND may not improve survival. The first aim of our study is to identify clinicopathological determinants associated with non-SN metastases. The second aim is to determine the impact of the number of sentinel node (SN) with macro-metastases and the type of SN metastases on metastatic involvement in non-SN.
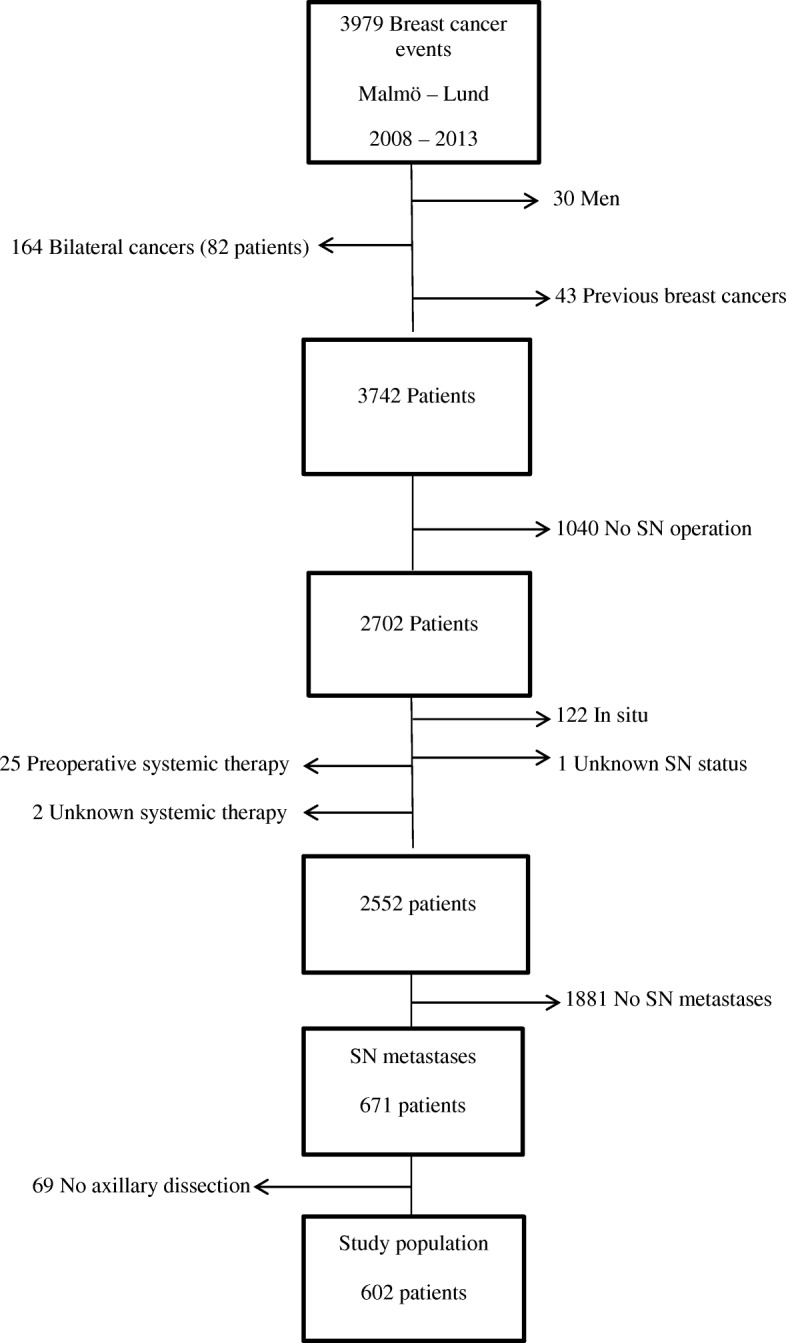
This is a retrospective study of 602 patients with primary invasive breast cancer operated on with SNB and c-ALND in Lund and Malmö during 2008-2013. All these patients had micro- and/or macro-metastases in SNs. Information was retrieved from the national Information Network for Cancer Care (INCA). The risk of metastases to non-SNs were analyzed in relation to clinicopathological determinants such as age, screening mammography, tumour size, tumour type, histological grade, estrogen status, progesterone status, HER2 status, multifocality and lymphovascular invasion. Additionally, we compared the association between the number of the SN and the type of metastases in SN with the risk of metastases to non-SNs. Binary logistic regression was used, yielding odds ratios (OR) with 95% confidence intervals (CI).
We found that 211 patients (35%) had metastases in non-SNs and 391 patients (65%) had no metastases in non-SNs. Lobular type (18%) of breast cancer (1.73; 1.0 1-2.97) and multifocal (31.3%) tumours (2.20; 1.41-3.44) had a high risk of non-SNs metastases. As compared to only micro-metastases, the presence of macro-metastases in SNs was associated with a high risk of metastases to non-SNs (4.91; 3.01-8.05). The number of SN with macro-metastases, regardless of the number of SNs removed by surgery, increases the risk of finding non-SNs with metastases. The total number of SN removed by surgery had no impact on diagnosis of metastases in non-SNs. No statistically significant associations were observed regarding other studied determinants.
We conclude in the present study that lobular cancer and multifocal tumours were associated with a high risk of non-SN involvement. The presence of the macro-metastases in SNs and the number of SN with macro-metastases has a positive association with presence of metastases in non-SNs. The total number of SNs removed by surgery had no impact on finding metastases in non-SNs. These factors may be valuable considering whether or not to omit c-ALND.
前哨淋巴结活检(SNB)是临床淋巴结阴性浸润性乳腺癌患者腋窝分期的标准程序。并非所有患者都需要进行完整的腋窝淋巴结清扫术(c-ALND),因为大量患者在非前哨淋巴结(非 SN)中没有进一步的转移,c-ALND 可能不会提高生存率。我们研究的第一个目的是确定与非 SN 转移相关的临床病理决定因素。第二个目的是确定 SN 中存在宏转移的 SN 数量和 SN 转移的类型对非 SN 转移的影响。
这是一项回顾性研究,纳入了 2008 年至 2013 年在隆德和马尔默接受 SNB 和 c-ALND 手术的 602 例原发性浸润性乳腺癌患者。所有这些患者的 SN 中均存在微转移和/或宏转移。信息从全国癌症护理信息网络(INCA)中检索。分析了年龄、筛查乳房 X 线摄影、肿瘤大小、肿瘤类型、组织学分级、雌激素状态、孕激素状态、HER2 状态、多灶性和脉管侵犯等临床病理决定因素与非 SN 转移风险之间的关系。此外,我们比较了 SN 中 SN 数量和转移类型与非 SN 转移风险之间的关联。使用二元逻辑回归,得出比值比(OR)及其 95%置信区间(CI)。
我们发现 211 例(35%)患者的非 SN 中有转移,391 例(65%)患者的非 SN 中无转移。乳腺癌症的小叶型(18%)(1.73;1.01-2.97)和多灶性(31.3%)肿瘤(2.20;1.41-3.44)有发生非 SN 转移的高风险。与仅存在微转移相比,SN 中存在宏转移与非 SN 转移的高风险相关(4.91;3.01-8.05)。SN 中存在宏转移的 SN 数量,而不考虑手术切除的 SN 数量,会增加发现非 SN 中有转移的风险。手术切除的 SN 总数对非 SN 中转移的诊断没有影响。关于其他研究的决定因素,未观察到统计学意义上的关联。
在本研究中,我们得出结论,小叶癌和多灶性肿瘤与非 SN 受累的高风险相关。SN 中的宏转移存在和 SN 中存在宏转移的数量与非 SN 中存在转移具有正相关性。手术切除的 SN 总数对非 SN 中转移的发现没有影响。这些因素对于是否省略 c-ALND 可能具有重要价值。