Department of Diagnostic and Interventional Radiology and Nuclear Medicine, University Hospital Hamburg-Eppendorf, Germany.
Department of General and Interventional Cardiology, University Heart Center, Germany.
Eur J Prev Cardiol. 2020 Jan;27(1):94-104. doi: 10.1177/2047487319859975. Epub 2019 Jun 26.
The aim of this study was to investigate the occurrence of myocardial injury and cardiac dysfunction after an endurance race by biomarkers and cardiac magnetic resonance in triathletes with and without myocardial fibrosis.
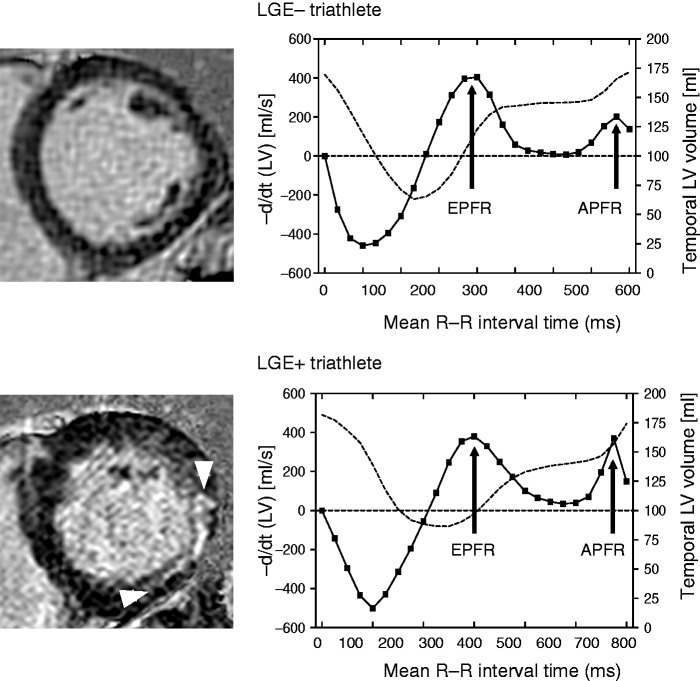
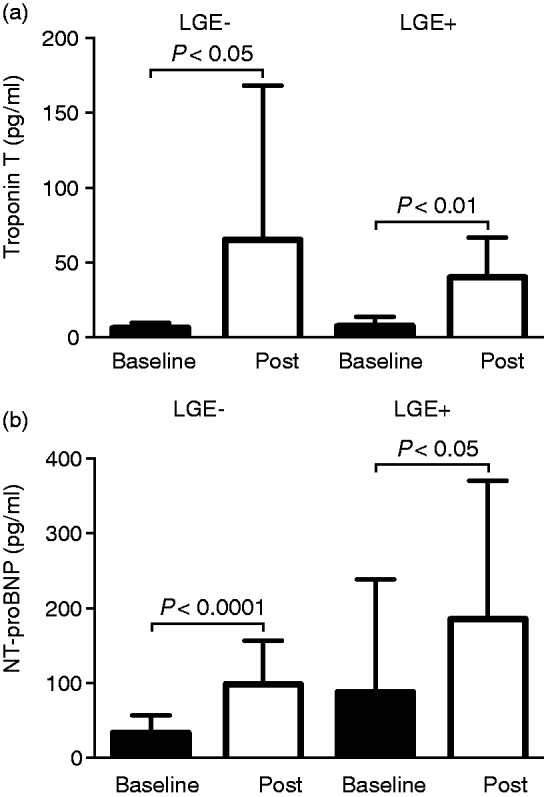
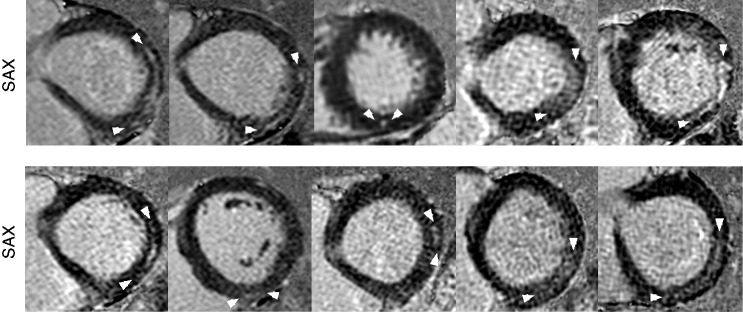
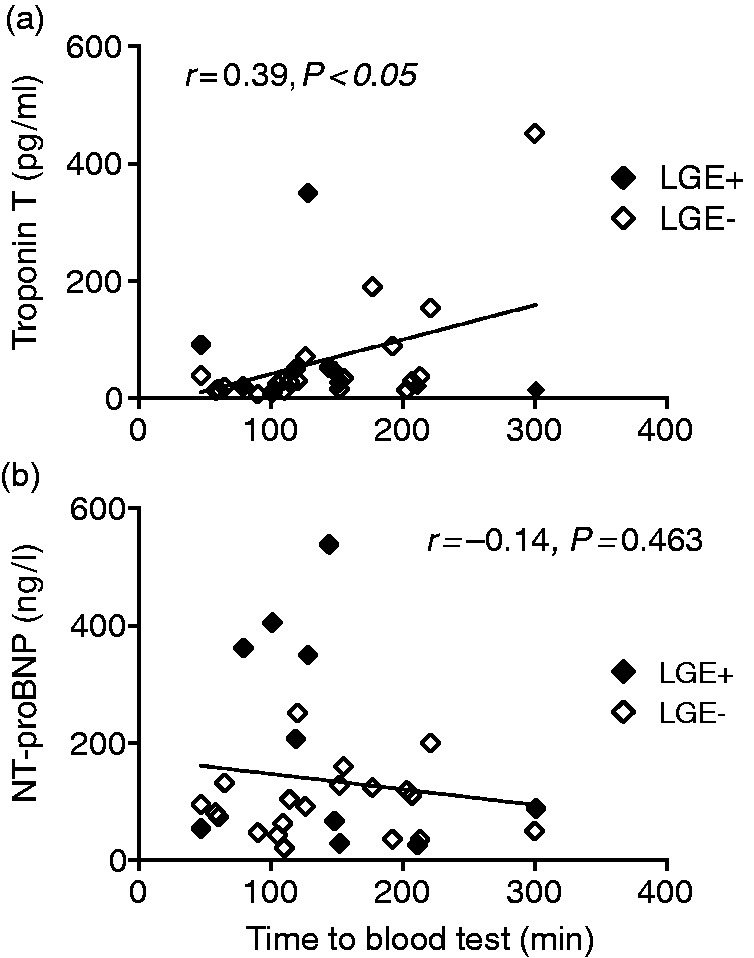
Thirty asymptomatic male triathletes (45 ± 10 years) with over 10 training hours per week and 55 ± 8 ml/kg per minute maximal oxygen uptake during exercise testing were studied before (baseline) and 2.4 ± 1.1 hours post-race. Baseline cardiac magnetic resonance included cine, T1/T2, late gadolinium enhancement (LGE) and extracellular volume imaging. Post-race non-contrast cardiac magnetic resonance included cine and T1/T2 mapping. Non-ischaemic myocardial fibrosis was present in 10 triathletes (LGE+) whereas 20 had no fibrosis (LGE-). At baseline, LGE + triathletes had higher peak exercise systolic blood pressure with 222 ± 21 mmHg compared to LGE- triathletes (192 ± 30 mmHg, < 0.01). Post-race troponin T and creatine kinase MB were similarly increased in both groups, but there was no change in T2 and T1 from baseline to post-race with 54 ± 3 ms versus 53 ± 3 ms ( = 0.797) and 989 ± 21 ms versus 989 ± 28 ms ( = 0.926), respectively. However, post-race left atrial ejection fraction was significantly lower in LGE + triathletes compared to LGE- triathletes (53 ± 6% vs. 59 ± 6%, < 0.05). Furthermore, baseline atrial peak filling rates were lower in LGE - triathletes (121 ± 30 ml/s/m) compared to LGE + triathletes (161 ± 34 ml/s/m, < 0.01). Post-race atrial peak filling rates increased in LGE- triathletes to 163 ± 46 ml/s/m, < 0.001), but not in LGE + triathletes (169 ± 50ml/s/m, = 0.747).
Despite post-race troponin T release, we did not find detectable myocardial oedema by cardiac magnetic resonance. However, the unfavourable blood pressure response during exercise testing seemed to be associated with post-race cardiac dysfunction, which could explain the occurrence of myocardial fibrosis in triathletes.
本研究旨在通过生物标志物和心脏磁共振检查,探讨有无心肌纤维化的耐力运动员赛后发生心肌损伤和心功能障碍的情况。
研究纳入了 30 名无症状的男性铁人三项运动员(45±10 岁),他们每周的训练时间超过 10 小时,运动试验中最大摄氧量为 55±8ml/kg/min。在比赛前(基线)和赛后 2.4±1.1 小时进行研究。基线心脏磁共振包括电影、T1/T2、晚期钆增强(LGE)和细胞外容积成像。赛后非对比心脏磁共振包括电影和 T1/T2 测绘。10 名运动员(LGE+)存在非缺血性心肌纤维化,20 名运动员(LGE-)无纤维化。在基线时,LGE+运动员的峰值运动收缩压更高,为 222±21mmHg,而 LGE-运动员为 192±30mmHg,差异有统计学意义( < 0.01)。两组运动员的赛后肌钙蛋白 T 和肌酸激酶 MB 均有相似的升高,但 T2 和 T1 从基线到赛后没有变化,分别为 54±3ms 与 53±3ms( = 0.797)和 989±21ms 与 989±28ms( = 0.926)。然而,LGE+运动员的赛后左心房射血分数明显低于 LGE-运动员(53±6% vs. 59±6%, < 0.05)。此外,LGE-运动员的基线心房峰值充盈率(121±30ml/s/m)低于 LGE+运动员(161±34ml/s/m, < 0.01)。LGE-运动员的赛后心房峰值充盈率增加到 163±46ml/s/m,差异有统计学意义( < 0.001),而 LGE+运动员则没有增加(169±50ml/s/m, = 0.747)。
尽管赛后肌钙蛋白 T 释放,但我们没有通过心脏磁共振检查发现可检测到的心肌水肿。然而,运动试验时的不良血压反应似乎与赛后心功能障碍有关,这可以解释铁人三项运动员中出现心肌纤维化的原因。