Ježek Filip, Strunina Svitlana, Carlson Brian E, Hozman Jiří
Department of Pathophysiology, First Faculty of Medicine, Charles University, Prague 2, Czech Republic.
Department of Molecular & Integrative Physiology, University of Michigan, Ann Arbor, MI, USA.
Int J Artif Organs. 2019 Dec;42(12):748-756. doi: 10.1177/0391398819858084. Epub 2019 Jun 27.
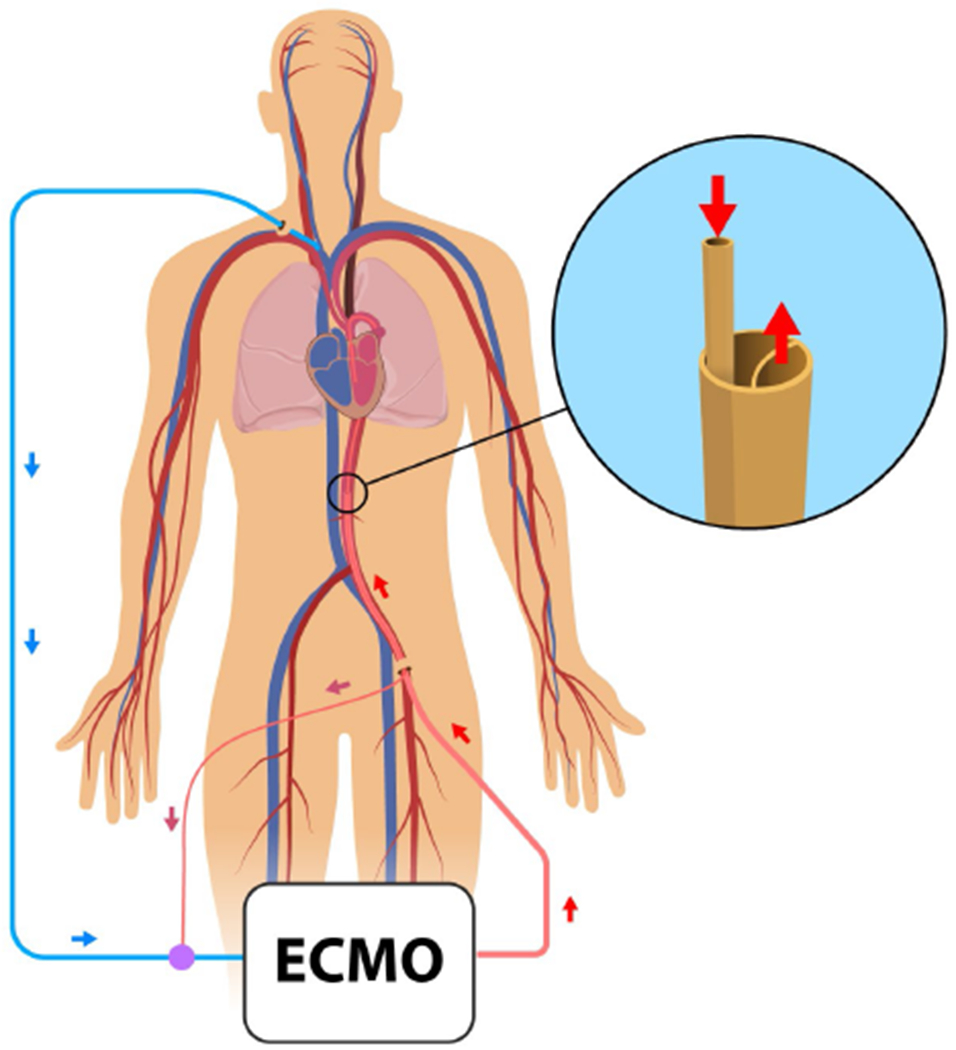
Veno-arterial extracorporeal membrane oxygenation can be vital to support patients in severe or rapidly progressing cardiogenic shock. In cases of left ventricular distension, left ventricular decompression during veno-arterial extracorporeal membrane oxygenation may be a crucial factor influencing the patient outcome. Application of a double lumen arterial cannula for a left ventricular unloading is an alternative, straightforward method for left ventricular decompression during extracorporeal membrane oxygenation in a veno-arterial configuration.
The purpose of this article is to use a mathematical model of the human adult cardiovascular system to analyze the left ventricular function of a patient in cardiogenic shock supported by veno-arterial extracorporeal membrane oxygenation with and without the application of left ventricular unloading using a novel double lumen arterial cannula.
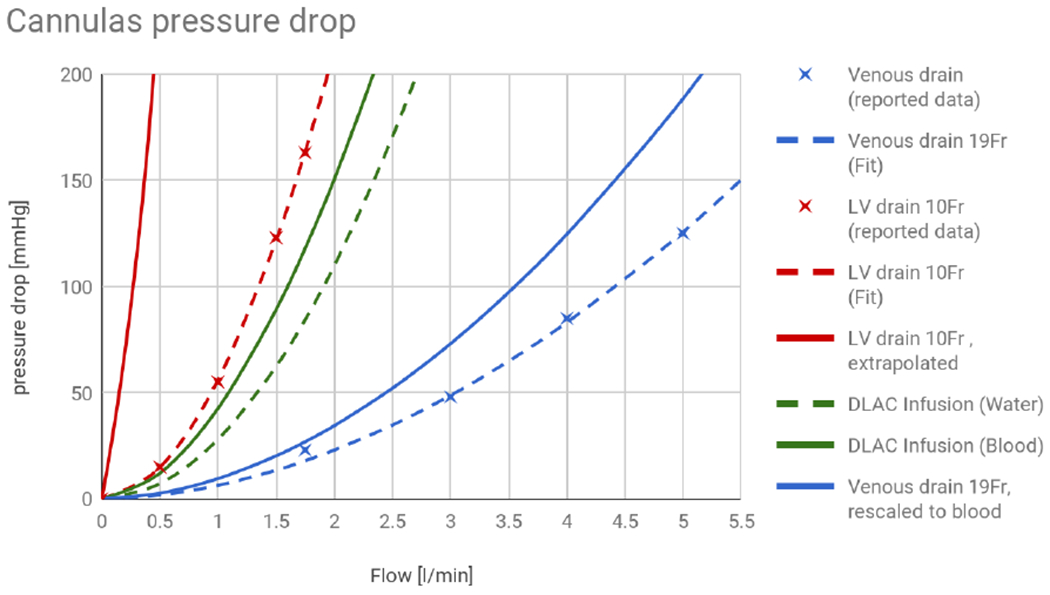
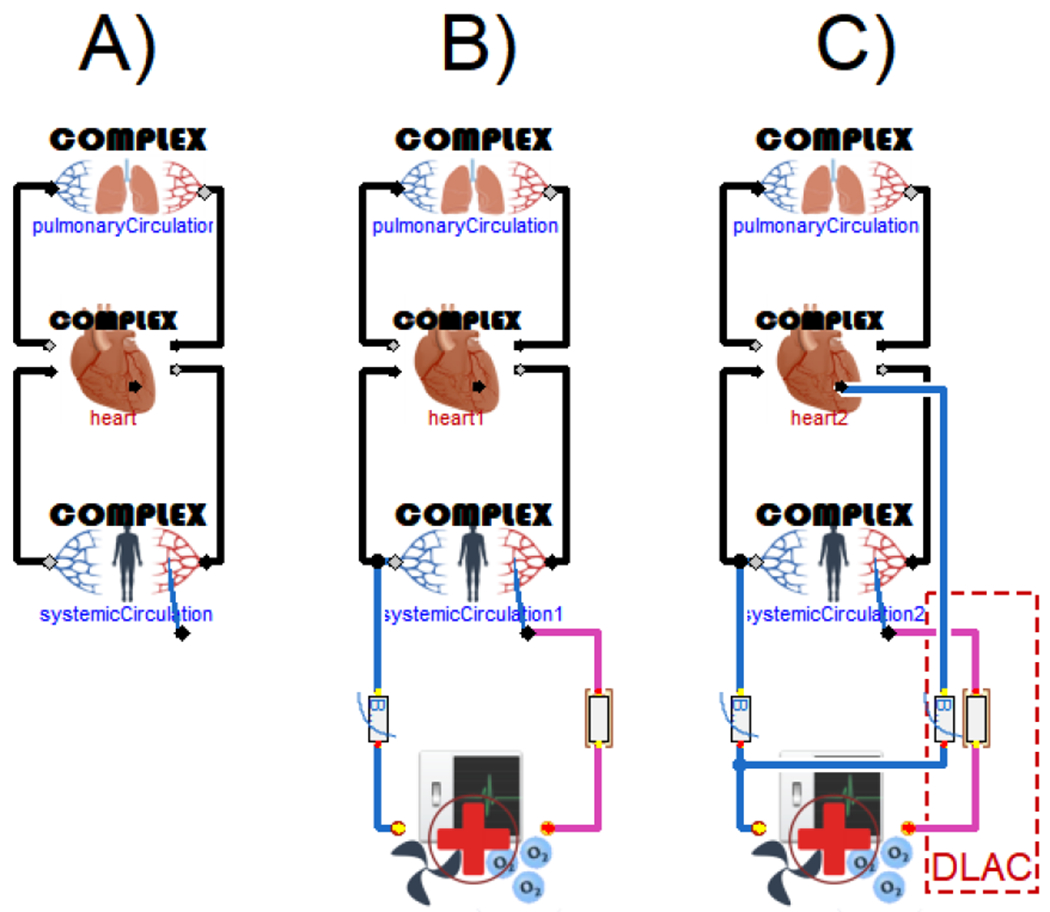
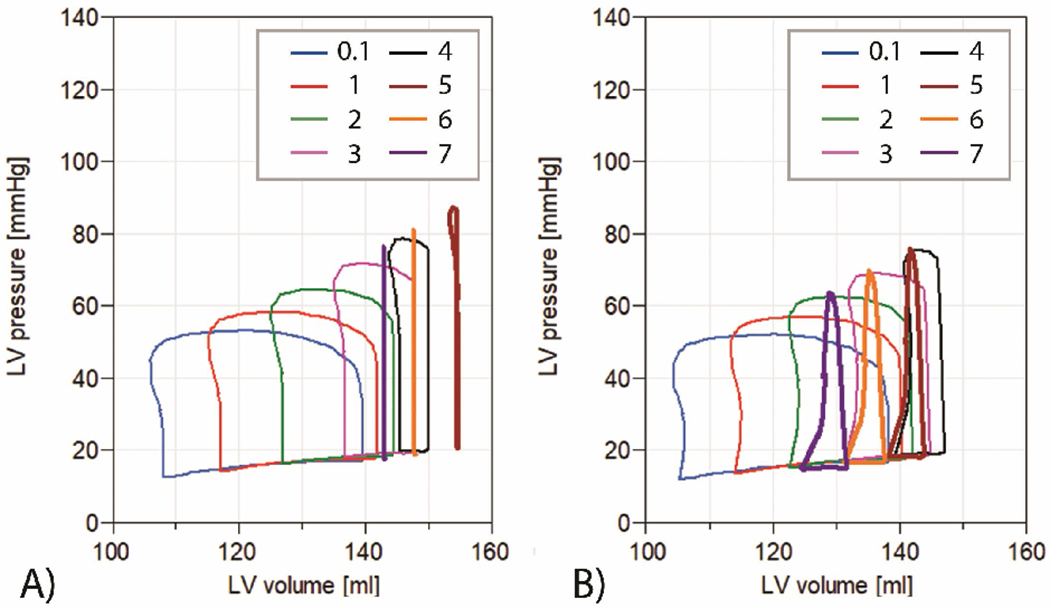
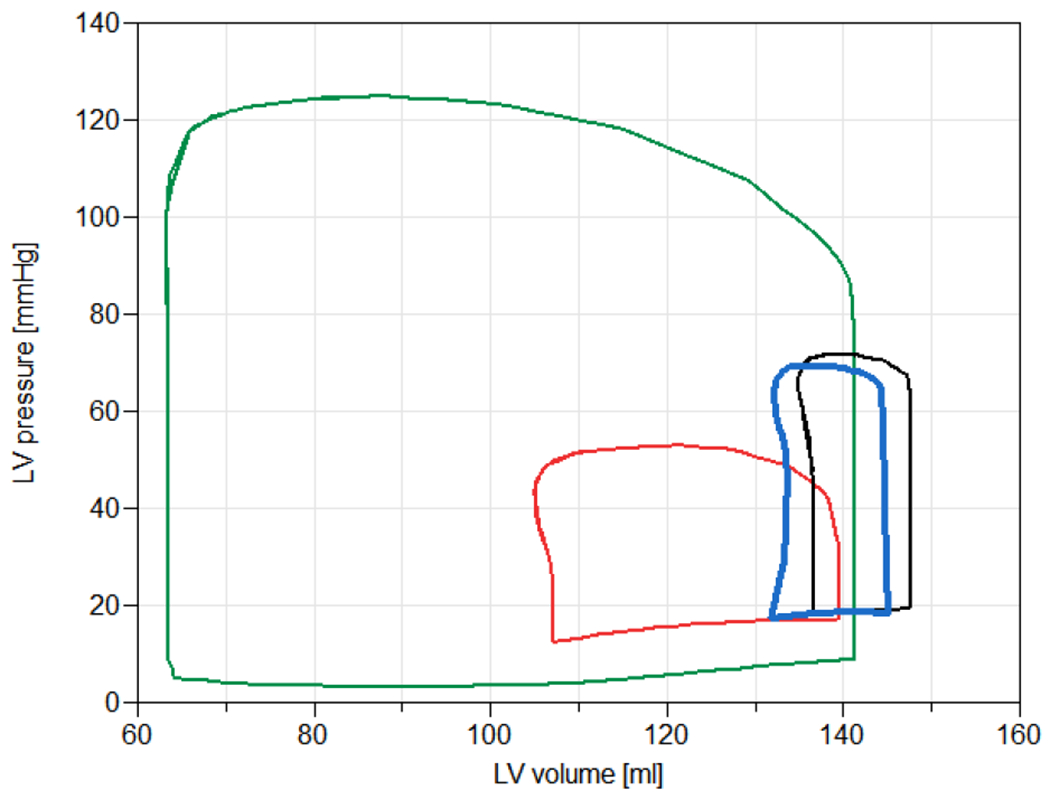
A lumped model of cardiovascular system hydraulics has been coupled with models of non-pulsatile veno-arterial extracorporeal membrane oxygenation, a standard venous cannula, and a drainage lumen of a double lumen arterial cannula. Cardiogenic shock has been induced by decreasing left ventricular contractility to 10% of baseline normal value.
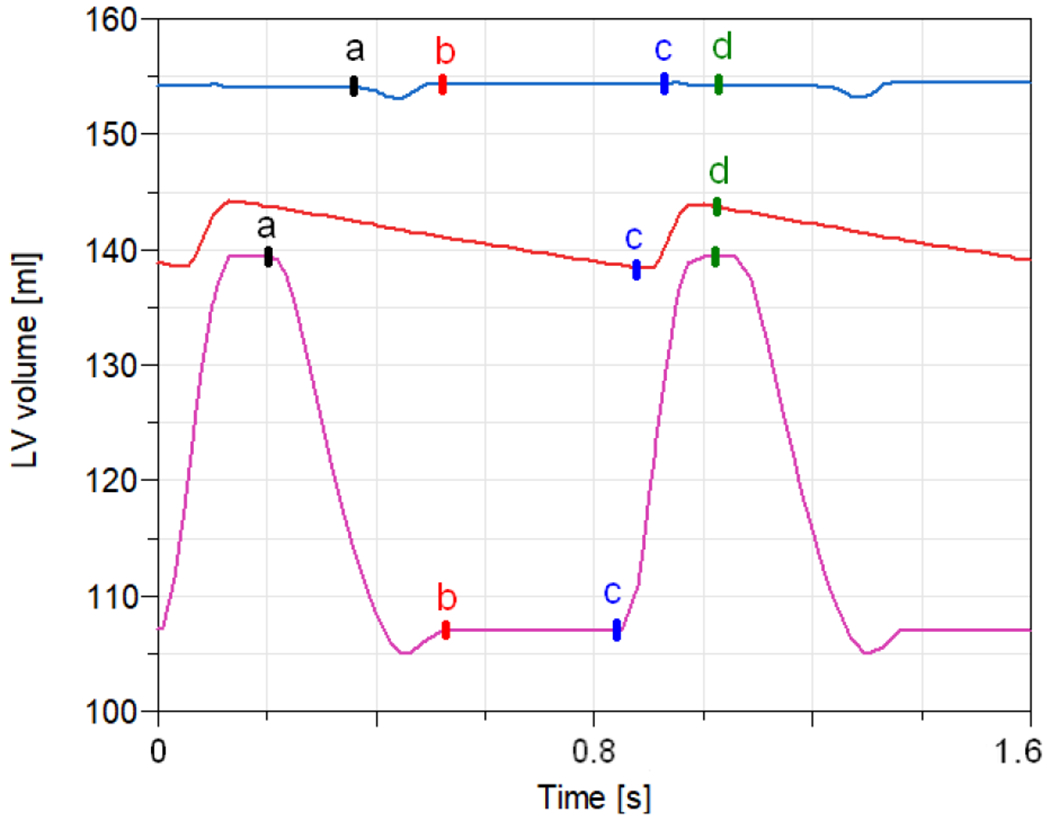
The simulation results indicate that applying double lumen arterial cannula during veno-arterial extracorporeal membrane oxygenation is associated with reduction of left ventricular end-systolic volume, end-diastolic volume, end-systolic pressure, and end-diastolic pressure.
A double lumen arterial cannula is a viable alternative less invasive method for left ventricular decompression during veno-arterial extracorporeal membrane oxygenation. However, to allow for satisfactory extracorporeal membrane oxygenation flow, the cannula design has to be revisited.
静脉-动脉体外膜肺氧合对于支持严重或快速进展的心源性休克患者至关重要。在左心室扩张的情况下,静脉-动脉体外膜肺氧合期间的左心室减压可能是影响患者预后的关键因素。应用双腔动脉插管进行左心室卸载是在静脉-动脉配置的体外膜肺氧合期间进行左心室减压的一种替代的、直接的方法。
本文的目的是使用成人人体心血管系统的数学模型,分析在静脉-动脉体外膜肺氧合支持下的心源性休克患者,在应用新型双腔动脉插管进行左心室卸载和未应用左心室卸载的情况下的左心室功能。
心血管系统液压集总模型已与非搏动性静脉-动脉体外膜肺氧合模型、标准静脉插管和双腔动脉插管的引流腔模型相结合。通过将左心室收缩力降低至基线正常值的10%来诱发心源性休克。
模拟结果表明,在静脉-动脉体外膜肺氧合期间应用双腔动脉插管与左心室收缩末期容积、舒张末期容积、收缩末期压力和舒张末期压力的降低有关。
双腔动脉插管是静脉-动脉体外膜肺氧合期间进行左心室减压的一种可行的、侵入性较小的替代方法。然而,为了实现满意的体外膜肺氧合流量,必须重新审视插管设计。