Department of of Gastroenterology, Infectious Diseases, and Rheumatology, Charite Universitatsmedizin Berlin, Berlin, Germany.
Rheumatology & Clinical Immunology, Academic Medical Center, University of Amsterdam, Amsterdam, The Netherlands.
RMD Open. 2019 Jun 7;5(1):e000917. doi: 10.1136/rmdopen-2019-000917. eCollection 2019.
This analysis assessed baseline predictors of remission in patients with non-radiographic axial spondyloarthritis (nr-axSpA) who received open-label adalimumab therapy.
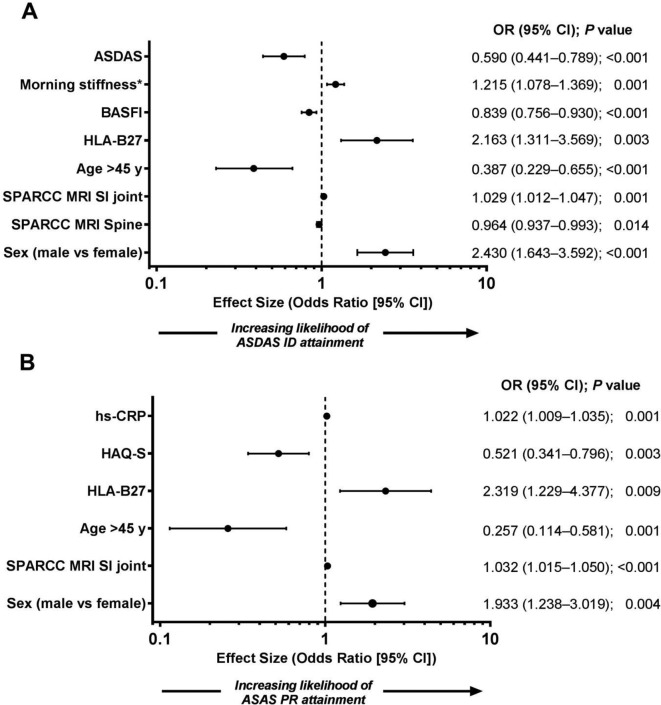
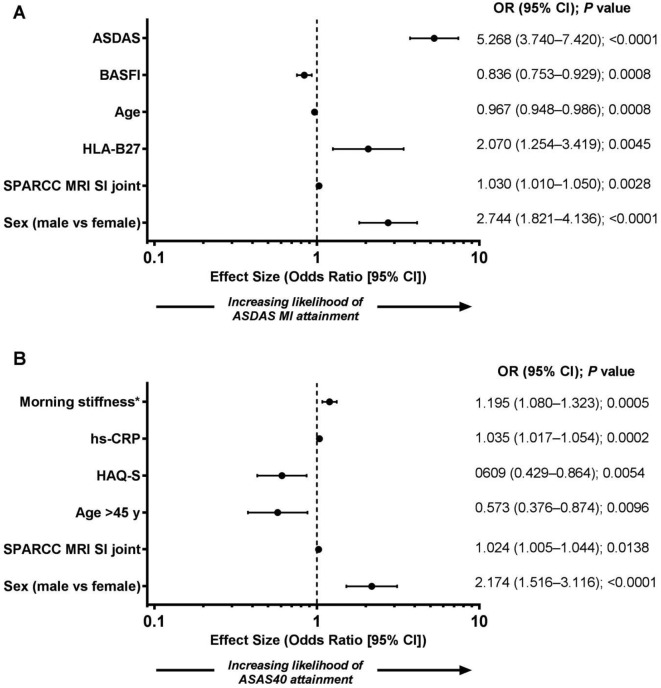
ABILITY-3 enrolled 673 adult patients with nr-axSpA who had objective evidence of inflammation by MRI or elevated high-sensitivity C reactive protein at screening, active disease and an inadequate response to two or more non-steroidal anti-inflammatory drugs. Patients received adalimumab 40 mg every other week during a 28-week open-label lead-in period. Clinical remission was defined as Ankylosing Spondylitis Disease Activity Score inactive disease (ASDAS ID; score <1.3) and Assessment of SpondyloArthritis international Society partial remission (ASAS PR; score <2/10 in each of the four ASAS domains). Stepwise logistic regression was used to identify baseline predictors of remission at week 12 and at final visit (last postbaseline visit up to week 28). Only patients without missing data were included.
Overall, 593 patients were included in the ASDAS ID and 596 in the ASAS PR analysis at week 12. Younger age (≤45 years), male sex, positive human leucocyte antigen (HLA)-B27 and higher Spondyloarthritis Research Consortium of Canada (SPARCC) MRI sacroiliac joint score were consistent predictors of remission by both ASAS ID and ASDAS PR at week 12. Results were generally similar in the final visit analysis. Other variables did not consistently predict remission.
In ABILITY-3, consistent and strong baseline predictors of remission included younger age, male sex, HLA-B27 positivity and higher SPARCC MRI sacroiliac joint score among patients with active nr-axSpA receiving adalimumab therapy, similar to previous findings in ankylosing spondylitis.
本分析评估了接受阿达木单抗开放标签治疗的非放射性轴性脊柱关节炎(nr-axSpA)患者的缓解的基线预测因子。
ABILITY-3 纳入了 673 名成年 nr-axSpA 患者,这些患者在筛查时具有 MRI 显示的炎症客观证据或高敏 C 反应蛋白升高,疾病处于活动期且对两种或多种非甾体抗炎药反应不足。患者在 28 周的开放标签导入期内每两周接受一次阿达木单抗 40mg 治疗。临床缓解定义为强直性脊柱炎疾病活动评分(ASDAS)无疾病活动(评分<1.3)和评估强直性脊柱炎国际协会部分缓解(ASAS PR;四个 ASAS 领域中每个领域的评分均<2/10)。逐步逻辑回归用于确定第 12 周和最终访视(最后一次基线后访视,直至第 28 周)时缓解的基线预测因子。仅纳入无缺失数据的患者。
总体而言,在第 12 周时,593 名患者纳入 ASDAS ID 分析,596 名患者纳入 ASAS PR 分析。年龄较小(≤45 岁)、男性、人类白细胞抗原(HLA)-B27 阳性和更高的 SPARCC 磁共振成像(MRI)骶髂关节评分是通过 ASAS ID 和 ASAS PR 在第 12 周时缓解的一致预测因子。最终访视分析的结果大致相似。其他变量并未一致预测缓解。
在 ABILITY-3 中,在接受阿达木单抗治疗的活动性 nr-axSpA 患者中,缓解的一致和强基线预测因子包括年龄较小、男性、HLA-B27 阳性和更高的 SPARCC MRI 骶髂关节评分,这与强直性脊柱炎的先前发现相似。