MMWR Morb Mortal Wkly Rep. 2019 Jul 5;68(26):577-582. doi: 10.15585/mmwr.mm6826a1.
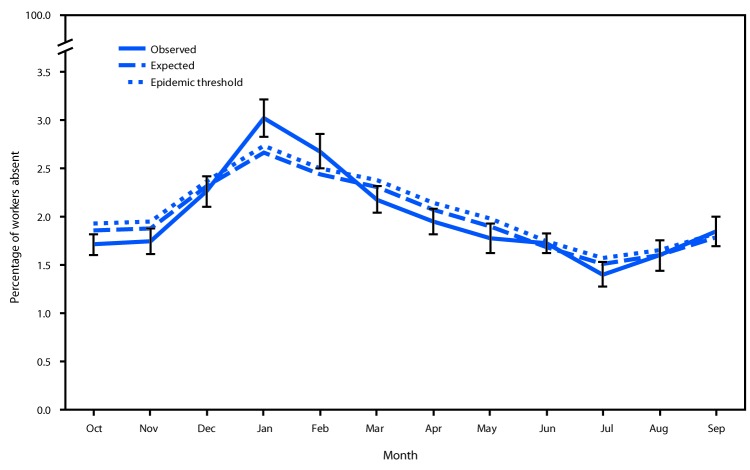
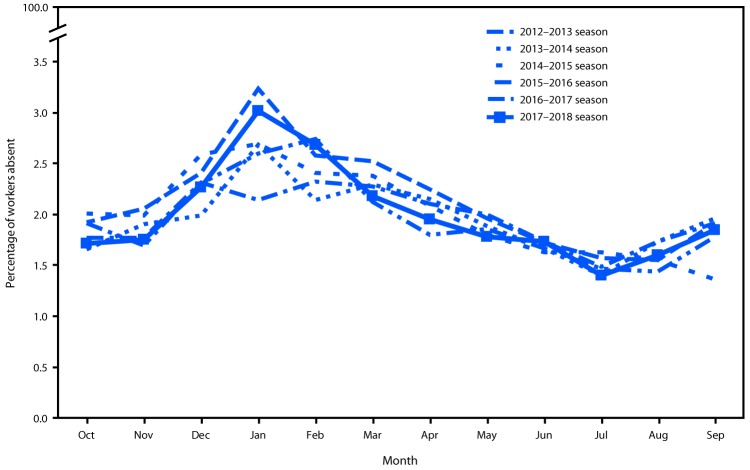
During an influenza pandemic and during seasonal epidemics, more persons have symptomatic illness without seeking medical care than seek treatment at doctor's offices, clinics, and hospitals (1). Consequently, surveillance based on mortality, health care encounters, and laboratory data does not reflect the full extent of influenza morbidity. CDC uses a mathematical model to estimate the total number of influenza illnesses in the United States (1). In addition, syndromic methods for monitoring illness outside health care settings, such as tracking absenteeism trends in schools and workplaces, are important adjuncts to conventional disease reporting (2). Every month, CDC's National Institute for Occupational Safety and Health (NIOSH) monitors the prevalence of health-related workplace absenteeism among full-time workers in the United States using data from the Current Population Survey (CPS) (3). This report describes the results of workplace absenteeism surveillance analyses conducted during the high-severity 2017-18 influenza season (October 2017-September 2018) (4). Absenteeism increased sharply in November, peaked in January and, at its peak, was significantly higher than the average during the previous five seasons. Persons especially affected included male workers, workers aged 45-64 years, workers living in U.S. Department of Health and Human Services (HHS) Region 6* and Region 9, and those working in management, business, and financial; installation, maintenance, and repair; and production and related occupations. Public health authorities and employers might consider results from relevant absenteeism surveillance analyses when developing prevention messages and in pandemic preparedness planning. The most effective ways to prevent influenza transmission in the workplace include vaccination and nonpharmaceutical interventions, such as staying home when sick, covering coughs and sneezes, washing hands frequently, and routinely cleaning frequently touched surfaces (5).
在流感大流行期间和季节性流行期间,有更多出现症状但未寻求医疗服务的人,而不是在医生办公室、诊所和医院寻求治疗(1)。因此,基于死亡率、医疗保健接触和实验室数据的监测并不能反映流感发病率的全部情况。CDC 使用数学模型来估计美国流感病例的总数(1)。此外,在医疗保健环境之外监测疾病的综合征方法,例如跟踪学校和工作场所的缺勤趋势,是常规疾病报告的重要辅助手段(2)。每月,CDC 的国家职业安全与健康研究所(NIOSH)使用来自当前人口调查(CPS)的数据监测美国全职工作者与健康相关的工作场所缺勤率(3)。本报告描述了在高严重度 2017-18 流感季节(2017 年 10 月至 2018 年 9 月)进行的工作场所缺勤监测分析的结果(4)。缺勤率在 11 月急剧上升,1 月达到峰值,且在峰值时明显高于过去五个季节的平均水平。受影响的人群包括男性工人、45-64 岁的工人、居住在卫生与公众服务部(HHS)第 6*区和第 9 区的工人,以及从事管理、商业和金融;安装、维护和修理;以及生产和相关职业的工人。公共卫生当局和雇主在制定预防信息和大流行准备计划时,可能会考虑相关缺勤监测分析的结果。在工作场所预防流感传播的最有效方法包括接种疫苗和非药物干预措施,例如生病时待在家里、咳嗽和打喷嚏时捂住口鼻、经常洗手以及定期清洁经常接触的表面(5)。