Center for Genomics and Systems Biology, Department of Biology, New York University, New York, NY, USA.
, Present Address: Memorial Sloan Kettering Cancer Center, 1275 York Avenue, New York, NY, USA.
BMC Infect Dis. 2019 Jul 3;19(1):572. doi: 10.1186/s12879-019-4161-6.
We conducted a diagnostic surveillance study to identify Plasmodium, dengue virus, chikungunya virus, and Orientia tsutsugamushi infections among febrile patients who underwent triage for malaria in the outpatient department at Ispat General Hospital, Rourkela, Odisha, India.
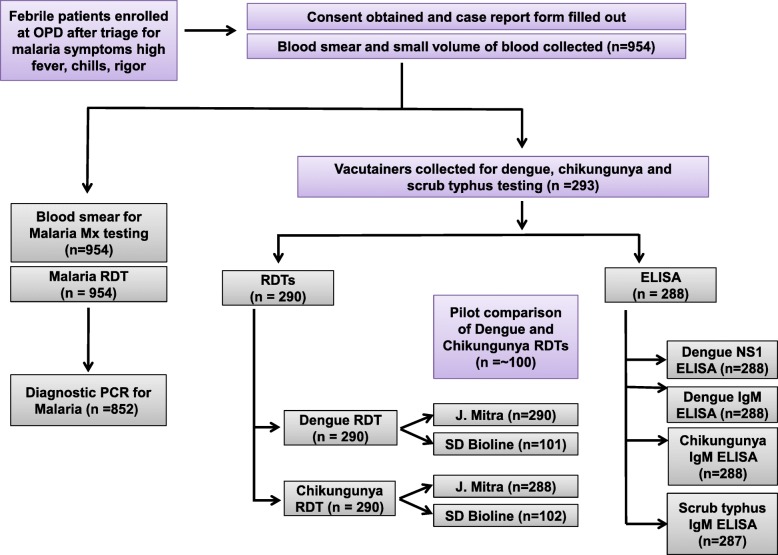
Febrile patients were enrolled from January 2016-January 2017. Blood smears and small volumes or vacutainers of blood were collected from study participants to carry out diagnostic assays. Malaria was diagnosed using rapid diagnostic tests (RDT), microscopy, and PCR. Dengue, chikungunya, and scrub typhus infections were identified using rapid diagnostic test kits and ELISA.
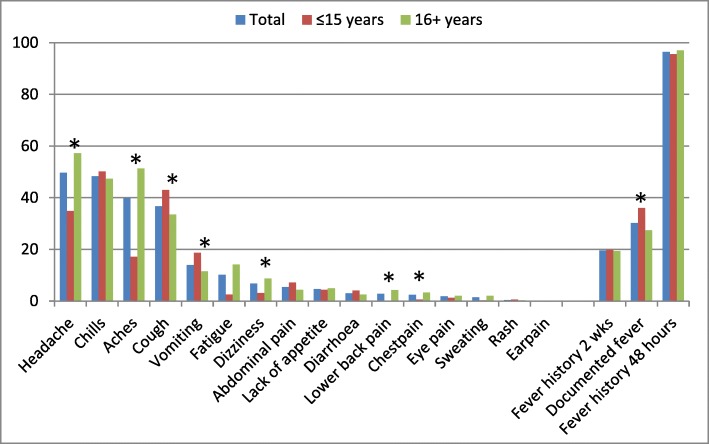
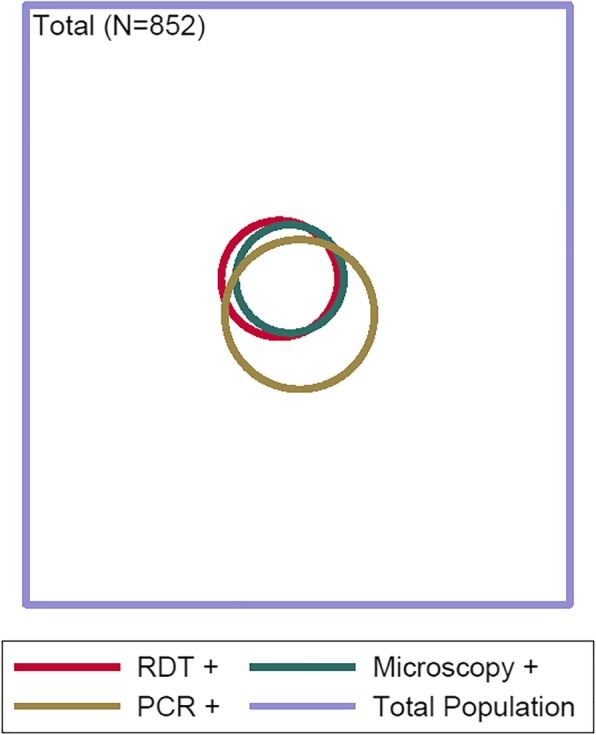
Nine hundred and fifty-four patients were prospectively enrolled in our study. The majority of patients were male (58.4%) and more than 15 years of age (66.4%). All 954 enrollees underwent additional testing for malaria; a subset of enrollees (293/954) that had larger volumes of plasma available was also tested for dengue, chikungunya and scrub typhus by either RDT or ELISA or both tests. Fifty-four of 954 patients (5.7%) were positive for malaria by RDT, or microscopy, or PCR. Seventy-four of 293 patients (25.3%) tested positive for dengue by either RDT or ELISA, and 17 of 293 patients (5.8%) tested positive for chikungunya-specific IgM by either ELISA or RDT. Ten of 287 patients tested (3.5%) were positive for scrub typhus by ELISA specific for scrub typhus IgM. Seventeen patients among 290 (5.9%) with results for ≥3 infections tested positive for more than one infection. Patients with scrub typhus and chikungunya had high rates of co-infection: of the 10 patients positive for scrub typhus, six were positive for dengue (p = 0.009), and five of 17 patients positive for chikungunya (by RDT or ELISA) were also diagnosed with malaria (p < 0.001).
Dengue, chikungunya and scrub typhus are important etiologies of non-malarial febrile illness in Rourkela, Odisha, and comorbidity should be considered. Routine febrile illness surveillance is required to accurately establish the prevalence of these infections in this region, to offer timely treatment, and to implement appropriate methods of control.
我们进行了一项诊断性监测研究,以鉴定印度奥里萨邦罗克尔 Ispat 综合医院门诊接受疟疾分诊的发热患者中的疟原虫、登革热病毒、基孔肯雅热病毒和恙虫病东方体感染。
2016 年 1 月至 2017 年 1 月期间,我们招募了发热患者。从研究参与者中采集血涂片和小体积或真空采血管的血液,以进行诊断检测。疟疾采用快速诊断检测(RDT)、显微镜检查和 PCR 进行诊断。使用快速诊断试剂盒和 ELISA 鉴定登革热、基孔肯雅热和恙虫病感染。
954 名患者前瞻性入组我们的研究。大多数患者为男性(58.4%),年龄超过 15 岁(66.4%)。所有 954 名入组患者均接受了疟疾的额外检测;其中一部分(293/954)有较大体积的血浆,也通过 RDT 或 ELISA 或两种检测方法进行了登革热、基孔肯雅热和恙虫病的检测。54 例(5.7%)患者 RDT、显微镜检查或 PCR 检测结果阳性。293 例患者中有 74 例(25.3%)通过 RDT 或 ELISA 检测结果阳性,293 例患者中有 17 例(5.8%)通过 ELISA 或 RDT 检测结果阳性基孔肯雅热特异性 IgM。287 例患者中有 10 例(3.5%)通过 ELISA 特异性检测恙虫病 IgM 检测结果阳性。290 例(5.9%)有≥3 种感染结果的患者中,有 17 例检测结果阳性。感染恙虫病和基孔肯雅热的患者合并感染率较高:10 例阳性的恙虫病患者中,6 例同时感染登革热(p=0.009),17 例通过 RDT 或 ELISA 检测结果阳性的基孔肯雅热患者中,有 5 例也诊断为疟疾(p<0.001)。
登革热、基孔肯雅热和恙虫病是奥里萨邦罗克尔发热性非疟疾的重要病因,应考虑合并感染。需要进行常规发热性疾病监测,以准确确定该地区这些感染的流行程度,提供及时治疗,并实施适当的控制方法。