Bilehjani Eissa, Fakhari Solmaz, Yaghoubi Alireza, Eslampoor Yashar, Atashkhoei Simin, Mirinajad Mousa
Departments of Anesthesiology, Tabriz University of Medical Sciences, Madani Heart Hospital, Tabriz, Iran.
Afr J Paediatr Surg. 2018 Apr-Jun;15(2):73-79. doi: 10.4103/ajps.AJPS_97_16.
The normal small difference (3-5 mmHg) between arterial (partial pressure of carbon dioxide [PaCO]) and end-tidal carbon dioxide pressure (ETPCO) increases in children with congenital heart disease. The present study was conducted to evaluate the effect of corrective or palliative cardiac surgery on this difference (known as DPCO2).
In a prospective study, 200 children (aged <12 years old) candidate for corrective or palliative cardiac surgery were studied. Using arterial blood gas measurement and simultaneous capnography, DPCO was calculated at various intra- and postoperative periods. DPCO values were compared within and between corrective or palliative procedures.
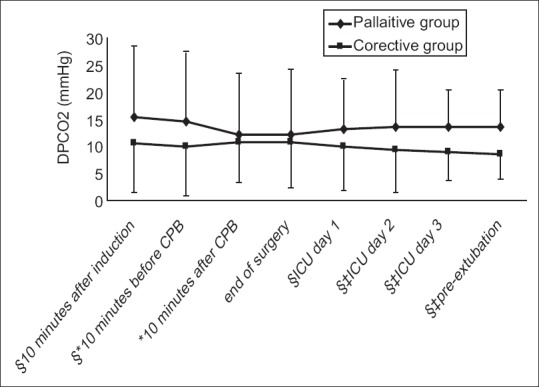
Corrective and palliative procedures were carried out on 154 and 46 patients, respectively. Initial DPCO was higher than normal values in corrective or palliative procedures (15.50 ± 13.1 and 10.75 ± 9.1 mmHg, respectively). DPCO was higher in patients who underwent palliative procedure, except early after procedure. The procedure did not have any effect on the final DPCO in palliative group. Although DPCO decrease was significant in the corrective group, it did not return to normal values. Operation time was longer, and the need to inotropic support was higher in corrective procedures; however, longer periods of ventilatory support were needed in the palliative group. Complication rate and Intensive Care Unit stay time were the same in two operation types.
DPCO did not change after palliative cardiac procedures. DPCO decreased after corrective procedures; however, it did not return to normal values at early postoperative period. Thus, DPCO may not have any clinical value in monitoring the quality of corrective or palliative procedures.
先天性心脏病患儿动脉血二氧化碳分压(PaCO₂)与呼气末二氧化碳分压(ETPCO₂)之间的正常微小差异(3 - 5 mmHg)会增大。本研究旨在评估心脏矫正或姑息手术对此差异(称为DPCO₂)的影响。
在一项前瞻性研究中,对200名(年龄<12岁)拟行心脏矫正或姑息手术的患儿进行了研究。通过动脉血气测量和同步二氧化碳描记法,在不同的术中及术后阶段计算DPCO。比较了矫正或姑息手术组内及组间的DPCO值。
分别对154例和46例患者进行了矫正和姑息手术。矫正或姑息手术中初始DPCO均高于正常值(分别为15.50 ± 13.1和10.75 ± 9.1 mmHg)。除术后早期外,姑息手术患者的DPCO更高。姑息手术组手术对最终DPCO无影响。虽然矫正组DPCO下降显著,但未恢复到正常值。矫正手术的手术时间更长,对血管活性药物支持的需求更高;然而,姑息手术组需要更长时间的通气支持。两种手术类型的并发症发生率和重症监护病房停留时间相同。
姑息性心脏手术后DPCO未改变。矫正手术后DPCO下降;然而,术后早期未恢复到正常值。因此,DPCO在监测矫正或姑息手术质量方面可能没有任何临床价值。