Department of Critical Care, Respiratory Institute, Cleveland Clinic, Cleveland, OH, USA.
Division of Critical Care Medicine, Department of Medicine, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand.
BMC Nephrol. 2019 Jul 10;20(1):255. doi: 10.1186/s12882-019-1439-2.
Acute kidney injury (AKI) is the most common extra-pulmonary organ failure in acute respiratory distress syndrome (ARDS). Renal recovery after AKI is determined by several factors. The objective of this study was to determine the predictors of renal non-recovery in ARDS patients.
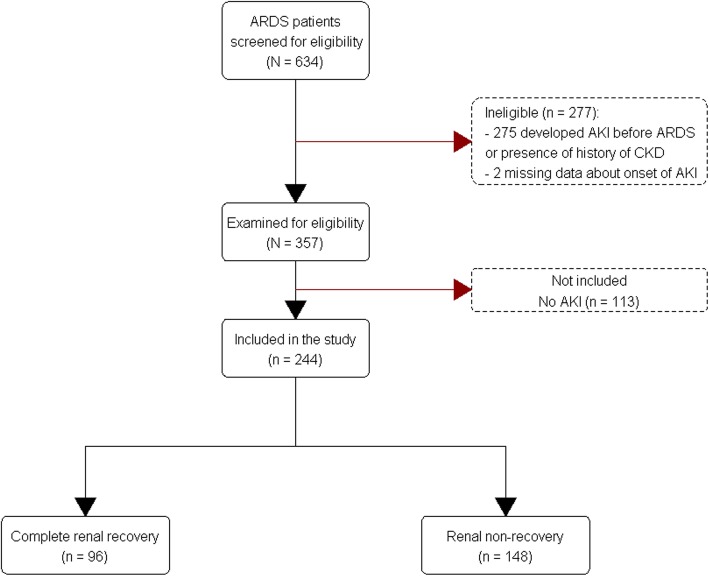
A single center retrospective cohort study of patients with AKI after onset of ARDS. Patients with preexisting chronic kidney disease or intensive care unit stay < 24 h were excluded. AKI staging was defined according to the Kidney Disease Improving Global Outcomes (KDIGO) 2012 guidelines. Renal non-recovery was defined as death, dialysis dependence, serum creatinine ≥1.5 times the baseline, or urine output < 0.5 mL/kg/h more than 6 h.
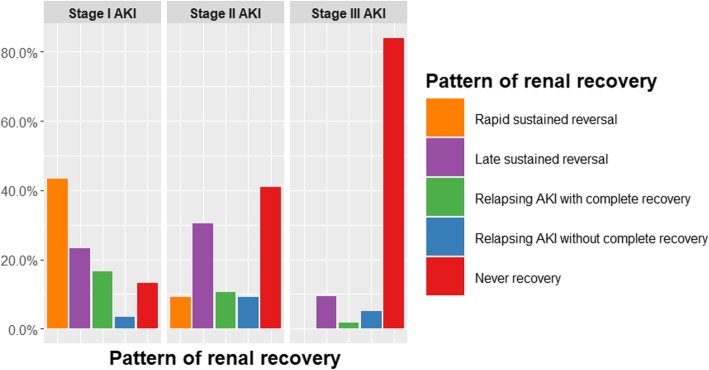
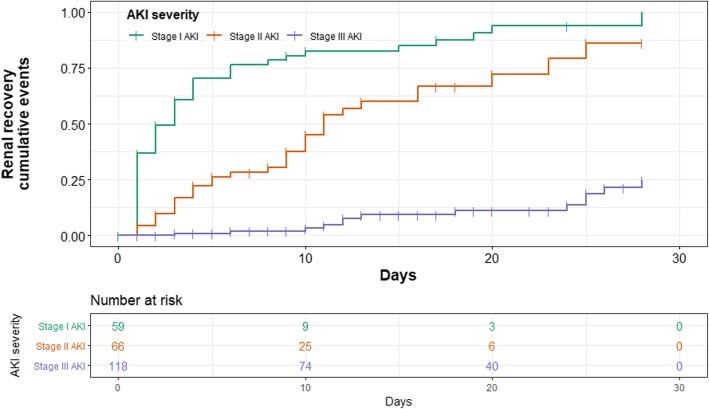
Of the 244 patients that met study criteria, 60 (24.6%) had stage I AKI, 66 (27%) had stage II AKI, and 118 (48.4%) had stage III AKI. Of those, 148 (60.7%) patients had renal non-recovery. On multivariable analysis, factors associated with renal non-recovery were a higher stage of AKI (odds ratio [OR] stage II 5.71, 95% confidence interval [CI] 2.17-14.98; OR stage III 45.85, 95% CI 16.27-129.2), delay in the onset of AKI (OR 1.12, 95% CI 1.03-1.21), history of malignancy (OR 4.02, 95% CI 1.59-10.15), septic shock (OR 3.2, 95% CI 1.52-6.76), and a higher tidal volume on day 1-3 of ARDS (OR 1.41, 95% CI 1.05-1.90). Subgroup analysis of survival at day 28 of ARDS also found that higher severity of AKI (OR stage II 8.17, 95% CI 0.84-79.91; OR stage III 111.67, 95% CI 12.69-982.91), delayed onset of AKI (OR 1.12, 95% CI 1.02-1.23), and active malignancy (OR 6.55, 95% CI 1.34-32.04) were significant predictors of renal non-recovery.
A higher stage of AKI, delayed onset of AKI, a history of malignancy, septic shock, and a higher tidal volume on day 1-3 of ARDS predicted renal non-recovery in ARDS patients. Among survivors, a higher stage of AKI, delayed onset of AKI, and a history of malignancy were associated with renal non-recovery.
急性肾损伤(AKI)是急性呼吸窘迫综合征(ARDS)中最常见的肺外器官衰竭。AKI 后的肾脏恢复由多个因素决定。本研究旨在确定 ARDS 患者肾功能无法恢复的预测因素。
这是一项对发生 ARDS 后出现 AKI 的患者进行的单中心回顾性队列研究。排除了患有慢性肾脏病或 ICU 入住时间 < 24 小时的患者。AKI 分期根据肾脏疾病改善全球结局(KDIGO)2012 指南定义。肾功能无法恢复定义为死亡、依赖透析、血清肌酐基线值的 1.5 倍以上,或 ARDS 发病后 1-3 天内的潮气量 1.41 倍,95%置信区间 1.05-1.90)。ARDS 发病后 1-3 天的较高潮气量(OR 1.41,95%CI 1.05-1.90)也与肾功能无法恢复相关。对 ARDS 发病后 28 天的生存情况进行亚组分析时,还发现 AKI 严重程度较高(OR 阶段 II 8.17,95%CI 0.84-79.91;OR 阶段 III 111.67,95%CI 12.69-982.91)、AKI 发病延迟(OR 1.12,95%CI 1.02-1.23)和活动性恶性肿瘤(OR 6.55,95%CI 1.34-32.04)是肾功能无法恢复的显著预测因素。
较高的 AKI 分期、AKI 发病延迟、恶性肿瘤病史、脓毒症休克和 ARDS 发病后 1-3 天的较高潮气量预测了 ARDS 患者的肾功能无法恢复。在幸存者中,较高的 AKI 分期、AKI 发病延迟和恶性肿瘤病史与肾功能无法恢复相关。