Searle Kendall, Blashki Grant, Kakuma Ritsuko, Yang Hui, Zhao Yuanlin, Minas Harry
1Global and Cultural Mental Health Unit, Centre for Mental Health, Melbourne School of Population and Global Health, University of Melbourne, Parkville, VIC 3010 Australia.
2Nossal Institute for Global Health, The University of Melbourne, Melbourne, VIC 3010 Australia.
Int J Ment Health Syst. 2019 Jun 28;13:47. doi: 10.1186/s13033-019-0300-0. eCollection 2019.
The prevalence of depressive disorder in Shenzhen is higher than for any other city in China. Despite national health system reform to integrate mental health into primary care, the majority of depression cases continue to go unrecognized and untreated. Qualitative research was conducted with primary care medical leaders to describe the current clinical practice of depressive disorder in community healthcare centres (CHC) in Shenzhen and to explore the participants' perceptions of psychological, organizational and societal barriers and enablers to current practice with a view to identifying current needs for the improved care of depressive disorder in the community.
Seventeen semi-structured, audio-recorded interviews (approx. 1 h long) were conducted in Melbourne (n = 7) and Shenzhen (n = 10) with a convenience sample of primary care medical leaders who currently work in community healthcare centres (CHC) in Shenzhen and completed any one of the 3-month long, Melbourne-based, "Monash-Shenzhen Primary Healthcare Leaders Programs" conducted between 2015 and 2017. The interview guide was developed using the Theoretical Domain's Framework (TDF) and a directed content analysis (using Nvivo 11 software) was performed using English translations.
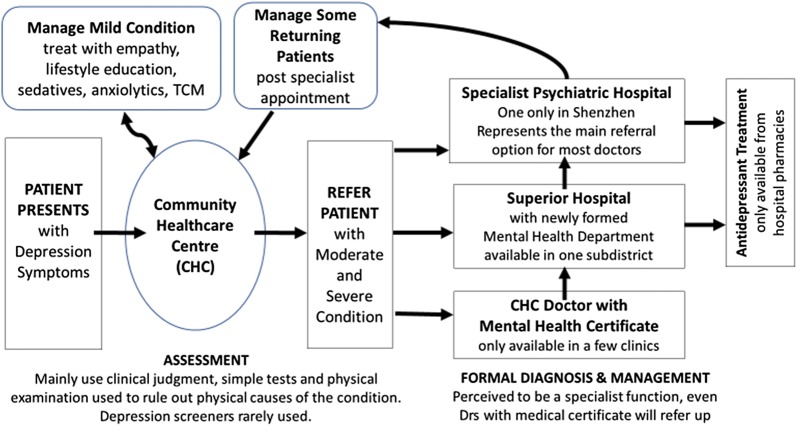
Despite primary care medical leaders being aware of a mental health treatment gap and the benefits of early depression care for community wellbeing, depressive disorder was not perceived as a treatment priority in CHCs. Instead, hospital specialists were identified as holding primary responsibility for formal diagnosis and treatment initiation with primary care doctors providing early assessment and basic health education. Current needs for improved depression care included: (i) Improved professional development for primary care doctors with better access to diagnostic guidelines and tools, case-sharing and improved connection with mentors to overcome current low levels of treatment confidence. (ii) An improved consulting environment (e.g. allocated mental health resource; longer and private consultations; developed medical referral system; better access to antidepressants) which embraces mental health initiatives (e.g. development of mental health departments in local hospitals; future use of e-mental health; reimbursement for patients; doctors' incentives). (iii) Improved health literacy to overcome substantive mental health stigma in society and specific stigma directed towards the only public psychiatric hospital.
Whilst a multi-faceted approach is needed to improve depression care in community health centres in Shenzhen, this study highlights how appropriate mental health training is central to developing a robust work-force which can act as key agents in national healthcare reform. The cultural adaption of the depression component of the World Health Organisation's mental health gap intervention guide (mhGAP-IG.v2) could provide primary care doctors with a future training tool to develop their assessment skills and treatment confidence.

深圳抑郁症的患病率高于中国其他任何城市。尽管国家进行了卫生系统改革,将心理健康纳入初级保健,但大多数抑郁症病例仍未得到识别和治疗。对初级保健医疗负责人进行了定性研究,以描述深圳社区医疗中心(CHC)目前对抑郁症的临床治疗情况,并探讨参与者对当前治疗中存在的心理、组织和社会障碍及促进因素的看法,以期确定当前社区改善抑郁症护理的需求。
在墨尔本(n = 7)和深圳(n = 10)对17名初级保健医疗负责人进行了半结构化的录音访谈(约1小时),这些负责人是从目前在深圳社区医疗中心工作且完成了2015年至2017年期间开展的为期3个月的墨尔本“莫纳什 - 深圳初级医疗保健领导者项目”中的任意一个项目的人员中便利抽样选取的。访谈指南是根据理论领域框架(TDF)制定的,并使用英语翻译进行了定向内容分析(使用Nvivo 11软件)。
尽管初级保健医疗负责人意识到心理健康治疗存在差距以及早期抑郁症护理对社区福祉的益处,但抑郁症在社区医疗中心并未被视为治疗重点。相反,医院专科医生被认为对正式诊断和开始治疗负有主要责任,初级保健医生则提供早期评估和基本健康教育。当前改善抑郁症护理的需求包括:(i)改善初级保健医生的专业发展,使其更容易获取诊断指南和工具、病例分享,并改善与导师的联系,以克服目前较低的治疗信心水平。(ii)改善咨询环境(例如分配心理健康资源;更长时间的私密咨询;完善的医疗转诊系统;更容易获取抗抑郁药),并接纳心理健康倡议(例如在当地医院设立精神科;未来使用电子心理健康服务;患者报销;医生激励措施)。(iii)提高健康素养,以克服社会上对心理健康的实质性污名以及针对唯一一家公立精神病医院的特定污名。
虽然需要采取多方面的方法来改善深圳社区卫生中心的抑郁症护理,但本研究强调了适当的心理健康培训对于培养一支强大的劳动力队伍至关重要,这支队伍可以成为国家医疗改革的关键力量。世界卫生组织心理健康差距干预指南(mhGAP - IG.v2)中抑郁症部分的文化适应性调整可以为初级保健医生提供一个未来的培训工具,以提高他们的评估技能和治疗信心。