Department of Internal Medicine, St Antonius Hospital, Koekoekslaan 1, 3435 CM, Nieuwegein, The Netherlands.
Dutch Kidney Patients Association (NVN), Bussum, The Netherlands.
BMC Nephrol. 2019 Jul 16;20(1):264. doi: 10.1186/s12882-019-1423-x.
Many older patients approaching end-stage kidney disease have to decide whether to go for dialysis or non-dialytic conservative care (CC). Shared decision-making is recommended to align the treatment plan with the patient's preferences and values. Little is known about older patients' experiences with shared decision-making on dialysis or CC.
We performed a survey study, in collaboration with the Dutch Kidney Patients Association, in 99 patients aged ≥70 years who had chosen dialysis (n = 75) or CC (n = 24) after a shared decision-making process involving an experienced multidisciplinary team.
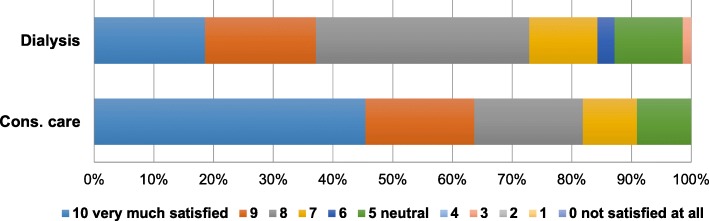
Patients stated to be overall satisfied with the shared decision-making process (% with score 6-10 on 11-point Likert scale, dialysis versus CC: 93% vs. 91%, P = 0.06), and treatment decision (87% vs. 91%, P = 0.03). However, patients also reported negative experiences, especially those who had chosen dialysis. Such negative experiences were related to the timing, informing, and level of decision-making being shared. More patients who selected dialysis indicated to have felt forced to make a decision, mostly due to the circumstances, such as their deteriorating health or kidney function, or by their nephrologist (31% vs. 5%, P = 0.01). Also, patients who selected dialysis mentioned a perceived lack of choice as most common reason for choosing dialysis, and 55% considered their own opinion as most important rather than their nephrologists' or relatives' opinion compared to 90% of the patients who had chosen CC (P = 0.02). A subset of patients who had chosen dialysis still doubted their treatment decision compared to no patient who had chosen CC (17% vs. 0%, P = 0.03).
Older patients reported contrasting experiences with shared decision-making on dialysis or CC. Despite high overall satisfaction, the underlying negative experiences illustrate important but modifiable barriers to an optimal shared decision-making process.
许多接近终末期肾病的老年患者必须决定是进行透析还是非透析保守治疗(CC)。建议进行共同决策,以使治疗计划与患者的偏好和价值观保持一致。对于老年患者在透析或 CC 方面的共同决策经验,知之甚少。
我们与荷兰肾脏患者协会合作,对 99 名年龄≥70 岁的患者进行了一项调查研究,这些患者在一个经验丰富的多学科团队参与的共同决策过程后选择了透析(n=75)或 CC(n=24)。
患者对共同决策过程总体表示满意(在 11 分李克特量表上得分 6-10 的比例,透析与 CC:93%与 91%,P=0.06),对治疗决策也表示满意(87%与 91%,P=0.03)。然而,患者也报告了一些负面体验,尤其是那些选择了透析的患者。这些负面体验与决策的时机、告知和共享程度有关。更多选择透析的患者表示感到被迫做出决定,主要是由于他们的健康或肾功能恶化等情况,或者是他们的肾病医生(31%与 5%,P=0.01)。此外,选择透析的患者提到缺乏选择是选择透析的最常见原因,与选择 CC 的患者相比,55%的患者认为自己的意见最重要,而不是他们的肾病医生或亲属的意见,而选择 CC 的患者中有 90%的人认为他们的肾病医生或亲属的意见最重要(P=0.02)。与选择 CC 的患者相比,选择透析的患者中有一小部分人仍然对他们的治疗决策表示怀疑(17%与 0%,P=0.03)。
老年患者在透析或 CC 方面的共同决策经验存在差异。尽管总体满意度较高,但潜在的负面体验说明了优化共同决策过程的重要但可改变的障碍。