Erasmus MC - Sophia Children's Hospital, University Medical Center Rotterdam, Rotterdam, the Netherlands.
Rady Children's Hospital, San Diego, CA, USA.
Dev Med Child Neurol. 2020 Jan;62(1):48-56. doi: 10.1111/dmcn.14306. Epub 2019 Jul 16.
To give evidence-based recommendations on the application of ketogenic diet parenteral nutrition (KD-PN) in emergency situations.
An international group of experts (n=14) researched the literature and distributed a survey among 150 expert centers. International accepted guidelines (European Society for Clinical Nutrition and Metabolism/European Society for Paediatric Gastroenterology Hepatology and Nutrition and the American Society for Parenteral and Enteral Nutrition) and handbooks for parenteral nutrition were considered general standards of care.
In the literature, we identified 35 reports of patients treated by KD-PN. International guidelines and handbooks provided some conflicting information. Twenty-four expert teams from nine countries responded to the survey, reflecting the limited clinical experience.
This paper highlights 23 consensus-based recommendations for safe and effective KD-PN (e.g. diet initiation, calculation, application, monitoring, and evaluation) based on the best evidence available and expert opinions.
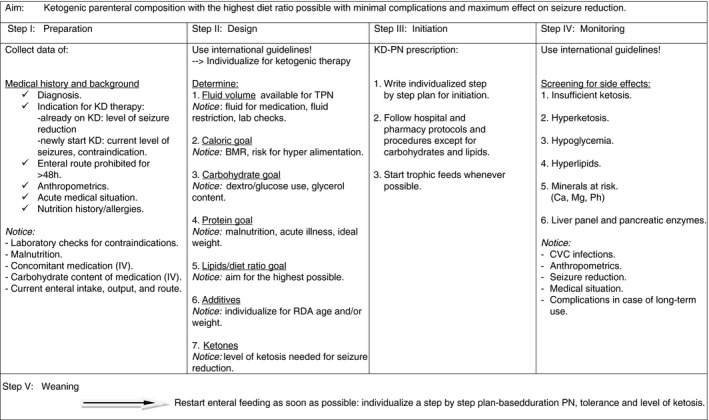
In acute settings, ketogenic diet therapy (KDT) can be administered parenterally. Parenteral administration of KDT should be started only at the intensive care unit. Initiate ketogenic parenteral nutrition stepwise to the highest ratio possible with the lowest level of complications. Evaluate the risk-benefit ratio of parenteral administration continuously. Restart enteral feeding as soon as appropriate.
为酮基饮食肠外营养(KD-PN)在紧急情况下的应用提供循证推荐意见。
一个由 14 名专家组成的国际专家组对文献进行了研究,并在 150 个专家中心进行了一项调查。国际公认的指南(欧洲临床营养与代谢学会/欧洲儿科胃肠病学、肝病学和营养学会和美国肠外和肠内营养学会)和肠外营养手册被视为一般护理标准。
在文献中,我们确定了 35 例接受 KD-PN 治疗的患者报告。国际指南和手册提供了一些相互矛盾的信息。来自九个国家的 24 个专家团队对调查做出了回应,反映了有限的临床经验。
本文根据现有最佳证据和专家意见,重点提出了 23 项关于 KD-PN 的安全有效共识推荐意见(如饮食起始、计算、应用、监测和评估)。
在急性情况下,可以给予酮基饮食治疗(KDT)肠外治疗。KDT 的肠外给药应仅在重症监护病房开始。逐步启动最高可能比例的酮基肠外营养,同时尽量降低并发症发生率。持续评估肠外给药的风险效益比。一旦合适,尽快重新开始肠内喂养。