Division of Neurology, Department of Medicine, St Michael's Hospital, University of Toronto, Toronto, Ontario, Canada.
Decision Neuroscience Unit, Li Ka Shing Knowledge Institute, St Michael's Hospital, University of Toronto, Toronto, Ontario, Canada.
JAMA Netw Open. 2019 Jul 3;2(7):e197093. doi: 10.1001/jamanetworkopen.2019.7093.
There is growing interest in understanding and addressing factors that govern the decision-making process in multiple sclerosis (MS) care. Therapeutic inertia (TI) is the failure to escalate therapy when goals are unmet. Limited data are available on the prevalence of TI and factors affecting therapeutic decisions in the management of patients with MS worldwide.
To compare TI across 4 countries (Canada, Argentina, Chile, and Spain) and to identify factors contributing to TI.
DESIGN, SETTING, AND PARTICIPANTS: Prospective cohort study conducted between July 10, 2017, and May 4, 2018. Participants were exposed to behavioral experiments in which instruments were used to assess their risk preferences (eg, aversion to ambiguity) and therapeutic decisions in 10 simulated MS case scenarios. Mixed-effects linear and logistic regression analyses were performed to determine the association between the participants' baseline characteristics and TI. The association of unmeasured confounders was assessed by the E-value and a bootstrapping analysis. This multicenter study included neurologists practicing at academic and community centers in Canada, Argentina, Chile, and Spain who make therapeutic decisions for patients with MS.
The primary outcome was the prevalence of TI. The TI score was calculated by dividing the number of case scenarios in which participants showed TI by the number of case scenarios that measured TI. Higher TI scores indicated greater degrees of TI. The secondary outcome was the identification of factors that contributed to TI.
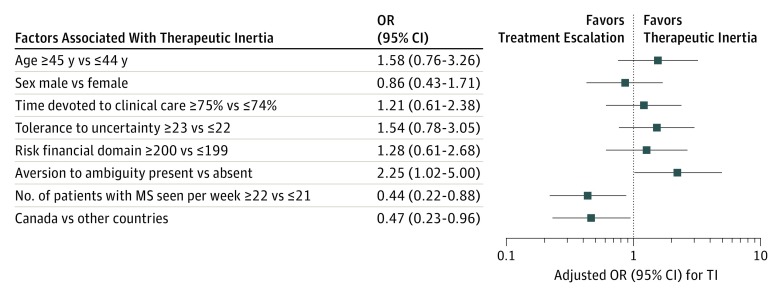
Of 300 neurologists with expertise in MS care who were invited to be part of the study, 226 (75.3%) agreed to participate. Among those who initially showed interest in participating, 195 physicians (86.3%) completed the study, while 31 did not. The mean (SD) age of participants was 43.3 (11.2) years; 52.3% were male. Therapeutic inertia was present in 72.8% (142 of 195) of participants, leading to suboptimal decisions in 20.4% (318 of 1560) of case scenarios. The prevalence of TI among the Canadian group was the lowest compared with the other 3 countries (60.0% [33 of 55] vs 77.9% [109 of 140]; P = .01). For the primary outcome, the TI score in the Canadian group (mean [SD], 0.98 [1.15]) was significantly lower compared with groups from other countries (mean [SD], 1.70 [1.43] for Argentina, 2.24 [1.54] for Chile, and 2.56 [1.64] for Spain) (P = .001). The mixed-effects linear models revealed that participants from Argentina, Chile, and Spain (combined) had higher TI scores compared with their Canadian counterparts (β coefficient, 0.90; 95% CI, 0.52-1.28; P < .001). A higher number of patients with MS per week (OR, 0.44; 95% CI, 0.22-0.88), years of practice (OR, 0.93; 95% CI, 0.86-0.99), and participation from Canada (OR, 0.47; 95% CI, 0.23-0.96) were associated with a lower likelihood of TI. Aversion to ambiguity was associated with a 2-fold higher likelihood of TI (OR, 2.25; 95% CI, 1.02-5.00). All 95% CIs of the β coefficients of covariates were lower than the E-value of 2.35, making it unlikely for the results to be due to the association of unmeasured confounders.
This study showed that Canadian participants had the lowest prevalence and magnitude of TI. Higher TI scores were associated with a lower expertise in MS care and with a greater tendency for aversion to ambiguity.
人们越来越关注理解和解决影响多发性硬化症(MS)护理决策的因素。治疗惰性(TI)是指当目标未实现时未能升级治疗。关于 TI 的流行率以及全球 MS 患者管理中影响治疗决策的因素,目前仅有有限的数据。
比较 4 个国家(加拿大、阿根廷、智利和西班牙)的 TI,并确定导致 TI 的因素。
设计、设置和参与者:这是一项于 2017 年 7 月 10 日至 2018 年 5 月 4 日进行的前瞻性队列研究。参与者接受了行为实验,其中使用仪器评估了他们的风险偏好(例如,对模糊性的厌恶)和 10 个模拟 MS 病例场景中的治疗决策。进行混合效应线性和逻辑回归分析,以确定参与者基线特征与 TI 之间的关联。通过 E 值和自举分析评估未测量混杂因素的关联。这项多中心研究包括在加拿大、阿根廷、智利和西班牙的学术和社区中心从事 MS 治疗决策的神经科医生。
主要结局是 TI 的流行率。TI 评分通过将参与者表现出 TI 的病例场景数除以测量 TI 的病例场景数来计算。较高的 TI 评分表示 TI 程度更高。次要结局是确定导致 TI 的因素。
在被邀请参与研究的 300 名精通 MS 护理的神经科医生中,有 226 名(75.3%)同意参与。在最初表现出参与兴趣的医生中,有 195 名(86.3%)完成了研究,而 31 名未完成。参与者的平均(SD)年龄为 43.3(11.2)岁;52.3%为男性。72.8%(142/195)的参与者存在 TI,导致 20.4%(318/1560)的病例场景做出了不理想的决策。与其他 3 个国家相比,加拿大组的 TI 流行率最低(60.0%[33/55]比 77.9%[109/140];P = .01)。对于主要结局,加拿大组的 TI 评分(均值[标准差],0.98[1.15])显著低于其他国家的评分(阿根廷组均值[标准差],1.70[1.43];智利组,2.24[1.54];西班牙组,2.56[1.64])(P = .001)。混合效应线性模型显示,来自阿根廷、智利和西班牙(合并)的参与者的 TI 评分高于他们的加拿大同行(β系数,0.90;95%置信区间,0.52-1.28;P < .001)。每周治疗的 MS 患者人数较多(比值比,0.44;95%置信区间,0.22-0.88)、从业年限较长(比值比,0.93;95%置信区间,0.86-0.99)和来自加拿大的参与(比值比,0.47;95%置信区间,0.23-0.96)与 TI 可能性较低相关。对模糊性的厌恶与 TI 可能性增加 2 倍相关(比值比,2.25;95%置信区间,1.02-5.00)。所有协变量的β系数的 95%置信区间均低于 2.35 的 E 值,表明结果不太可能是由于未测量混杂因素的关联所致。
本研究表明,加拿大参与者的 TI 流行率和程度最低。较高的 TI 评分与 MS 护理专业知识较低以及对模糊性的厌恶程度较高有关。