Department of Colorectal Surgery, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Bejing, China.
Department of Anesthesiology, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Bejing, China.
BMC Cancer. 2019 Jul 17;19(1):704. doi: 10.1186/s12885-019-5912-x.
The early detection of synchronous bone metastasis (BM) in newly diagnosed colorectal cancer (CRC) affects its initial management and prognosis. A clinical model to individually predict the risk of developing BM would be attractive in current clinical practice.
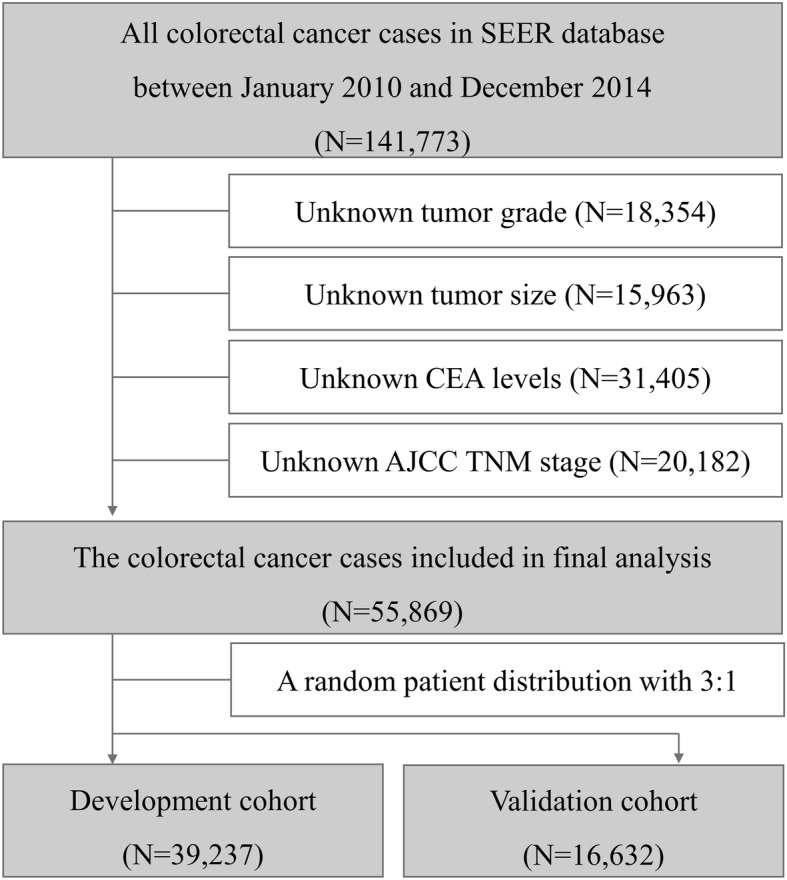
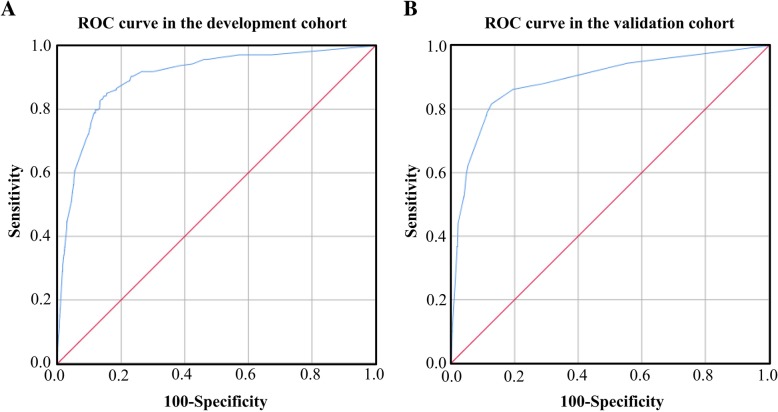
A total of 55,869 CRC patients were identified from Surveillance, Epidemiology, and End Results (SEER) database, of whom 317 patients were diagnosed with synchronous BM. Risk factors for BM in CRC patients was identified using multivariable logistic regression. A weighted scoring system was built with beta-coefficients (P < 0.05). A random sample of 75% of the CRC patients was used to establish the risk model, and the remaining 25% was used to validate its accuracy of this model. The performance of risk model was estimated by receiver operating curve (ROC) analysis.
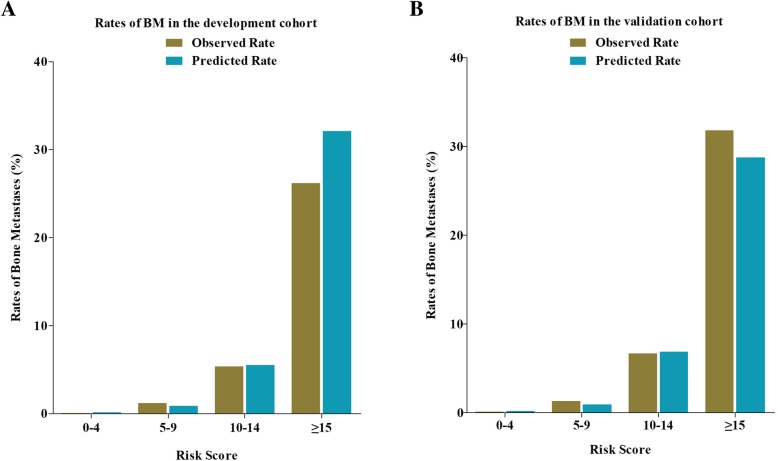
The risk model consisted of 8 risk factors including rectal cancer, poorly-undifferentiation, signet-ring cell carcinoma, CEA positive, lymph node metastasis, brain metastasis, liver metastasis and lung metastasis. The areas under the receiver operating curve (AUROC) were 0.903 and 0.889 in the development and validation cohort. Patients with scores from 0 to 4 points had about 0.1% risk of developing BM, and the risk increased to about 30% in patients with scores ≥15 points.
This clinical risk model is accurate enough to identify the CRC patients with high risk of synchronous BM and to further provide more individualized clinical decision.
在新诊断的结直肠癌(CRC)中早期发现同步骨转移(BM)会影响其初始管理和预后。在当前的临床实践中,建立一种能够个体化预测 BM 发生风险的临床模型将是非常有吸引力的。
从监测、流行病学和最终结果(SEER)数据库中确定了 55869 例 CRC 患者,其中 317 例被诊断为同步 BM。使用多变量逻辑回归确定 CRC 患者发生 BM 的危险因素。使用 beta 系数(P < 0.05)构建加权评分系统。CRC 患者的 75%随机样本用于建立风险模型,其余 25%用于验证该模型的准确性。通过接受者操作特征(ROC)曲线分析来评估风险模型的性能。
该风险模型由 8 个危险因素组成,包括直肠癌、低分化、印戒细胞癌、CEA 阳性、淋巴结转移、脑转移、肝转移和肺转移。在开发和验证队列中,该风险模型的 ROC 曲线下面积(AUROC)分别为 0.903 和 0.889。评分在 0 到 4 分的患者发生 BM 的风险约为 0.1%,而评分≥15 分的患者的风险增加到约 30%。
该临床风险模型具有足够的准确性,可以识别出发生同步 BM 的 CRC 患者,为进一步提供更个体化的临床决策提供依据。