Department of Immunology, Mayo Clinic, Rochester, MN, 55905, USA.
Medical Scientist Training Program, Mayo Clinic, Rochester, MN, 55905, USA.
J Immunother Cancer. 2019 Jul 17;7(1):188. doi: 10.1186/s40425-019-0673-2.
Immunotherapy has shown remarkable clinical promise in the treatment of various types of cancers. However, clinical benefits derive from a highly inflammatory mechanism of action. This presents unique challenges for use in pediatric brainstem tumors including diffuse intrinsic pontine glioma (DIPG), since treatment-related inflammation could cause catastrophic toxicity. Therefore, the goal of this study was to investigate whether inflammatory, immune-based therapies are likely to be too dangerous to pursue for the treatment of pediatric brainstem tumors.
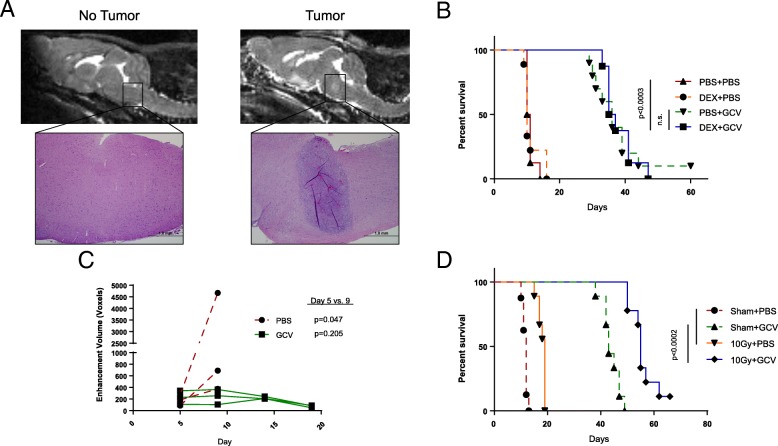
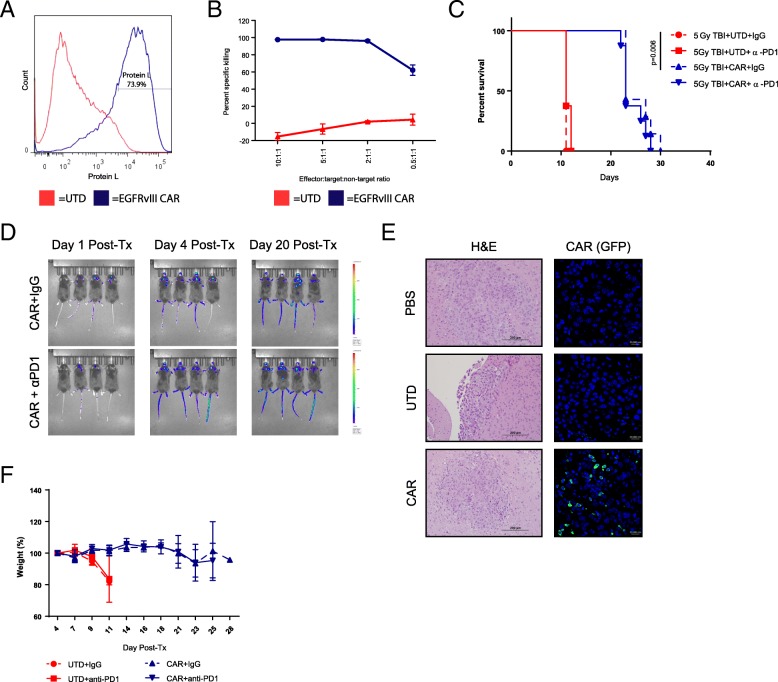
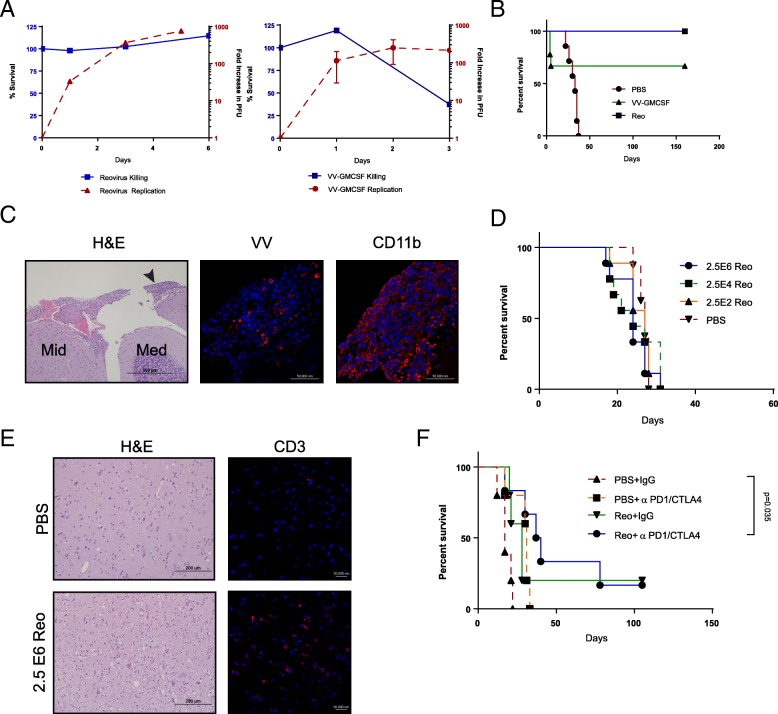
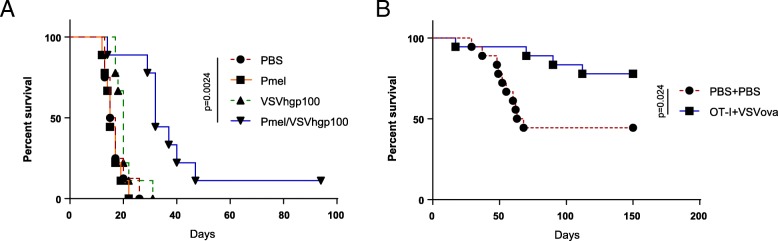
To complement previous immunotherapy studies using patient-derived xenografts in immunodeficient mice, we developed fully immunocompetent models of immunotherapy using transplantable, syngeneic tumors. These four models - HSVtk/GCV suicide gene immunotherapy, oncolytic viroimmunotherapy, adoptive T cell transfer, and CAR T cell therapy - have been optimized to treat tumors outside of the CNS and induce a broad spectrum of inflammatory profiles, maximizing the chances of observing brainstem toxicity.
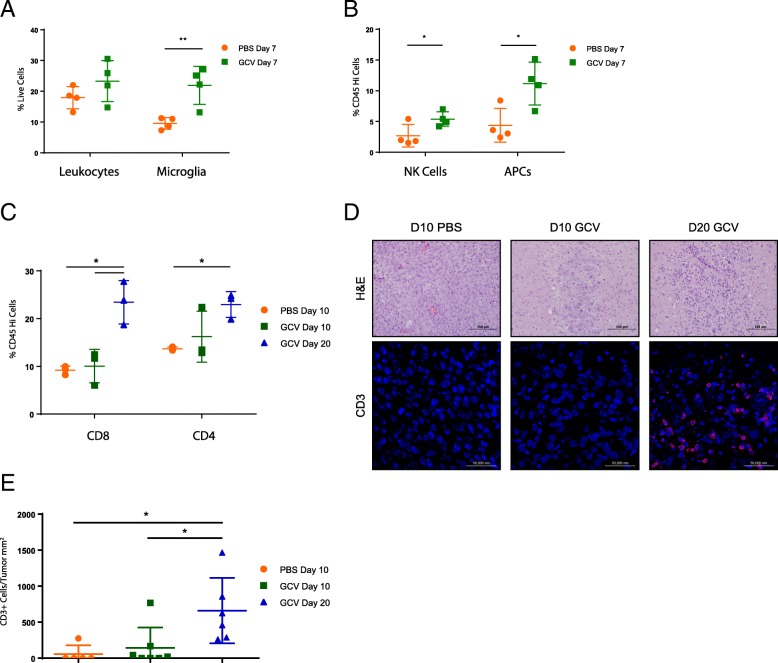
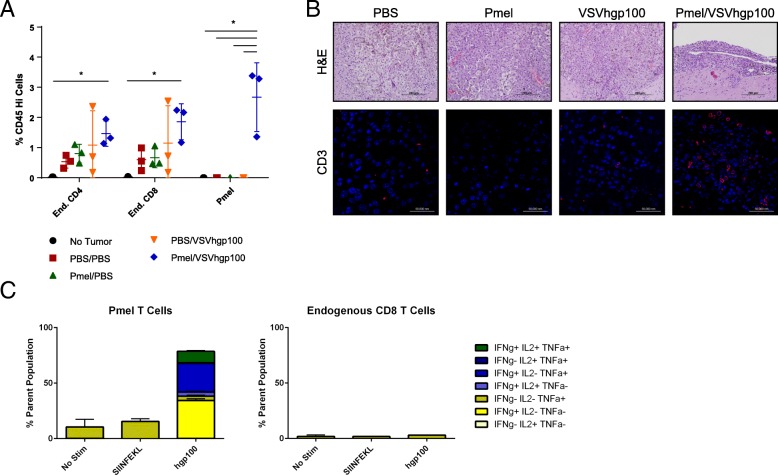
All four models achieved anti-tumor efficacy in the absence of toxicity, with the exception of recombinant vaccinia virus expressing GMCSF, which demonstrated inflammatory toxicity. Histology, imaging, and flow cytometry confirmed the presence of brainstem inflammation in all models. Where used, the addition of immune checkpoint blockade did not introduce toxicity.
It remains imperative to regard the brainstem with caution for immunotherapeutic intervention. Nonetheless, we show that further careful development of immunotherapies for pediatric brainstem tumors is warranted to harness the potential potency of anti-tumor immune responses, despite their possible toxicity within this anatomically sensitive location.
免疫疗法在治疗各种类型的癌症方面显示出显著的临床前景。然而,临床获益源于一种高度炎症的作用机制。这为在儿科脑干肿瘤(包括弥漫性内在脑桥胶质瘤[DIPG])中使用带来了独特的挑战,因为治疗相关的炎症可能导致灾难性的毒性。因此,本研究的目的是探讨炎症性、基于免疫的疗法是否可能因对儿科脑干肿瘤的治疗过于危险而无法进行。
为了补充以前在免疫缺陷小鼠中使用患者来源的异种移植物进行的免疫疗法研究,我们开发了使用可移植的同源肿瘤的完全免疫相容模型。这四种模型 - HSVtk/GCV 自杀基因免疫疗法、溶瘤病毒免疫疗法、过继性 T 细胞转移和 CAR T 细胞疗法 - 已被优化用于治疗 CNS 以外的肿瘤,并诱导广泛的炎症谱,最大限度地观察到脑干毒性的机会。
除了表达 GMCSF 的重组痘苗病毒外,所有四种模型在没有毒性的情况下都实现了抗肿瘤疗效,该病毒表现出炎症毒性。组织学、影像学和流式细胞术证实了所有模型中均存在脑干炎症。在使用的情况下,添加免疫检查点阻断并不会引入毒性。
对于免疫治疗干预,仍然必须谨慎对待脑干。尽管如此,我们表明,需要进一步谨慎地开发儿科脑干肿瘤的免疫疗法,以利用抗肿瘤免疫反应的潜在效力,尽管它们在这个解剖学上敏感的位置可能具有毒性。