Brotherton Julia Ml, Budd Alison, Rompotis Christopher, Bartlett Natasha, Malloy Michael J, Andersen Rachael L, Coulter Kim Ar, Couvee Peter W, Steel Nerida, Ward Gail H, Saville Marion
National HPV Vaccination Program Register, VCS Population Health, VCS Foundation, East Melbourne, Victoria, Australia; Melbourne School of Population and Global Health, University of Melbourne, Victoria, Australia.
Screening Analysis and Monitoring Unit, Australian Institute of Health and Welfare, Canberra, Australia.
Papillomavirus Res. 2019 Dec;8:100177. doi: 10.1016/j.pvr.2019.100177. Epub 2019 Jul 15.
Prophylactic human papillomavirus (HPV) vaccines are highly effective at preventing pre-cancerous cervical lesions when given in a three-dose schedule. Some post-hoc trial data suggest that one dose prevents HPV infection. If one dose could prevent pre-cancerous cervical lesions, then global cervical cancer prevention would be greatly facilitated. We assessed the effectiveness of quadrivalent HPV vaccine by number of doses against cervical intraepithelial neoplasia (CIN) 2 or 3/adenocarcinoma-in-situ (AIS)/cancer in Australia up to seven years post vaccination.
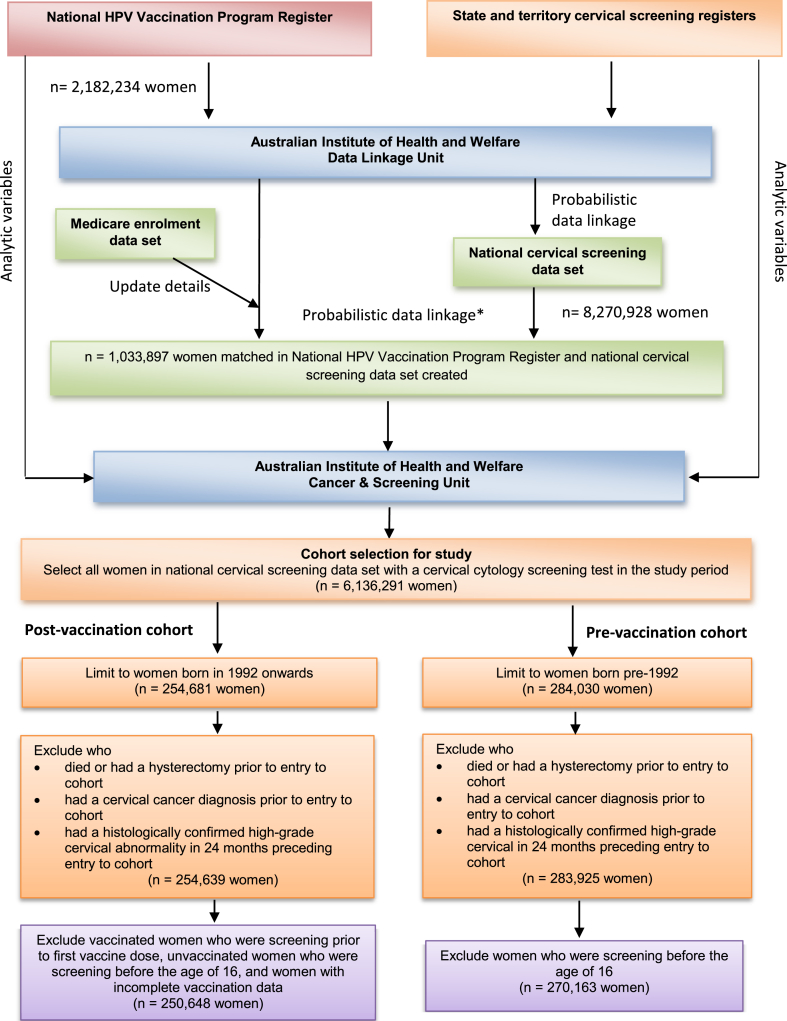
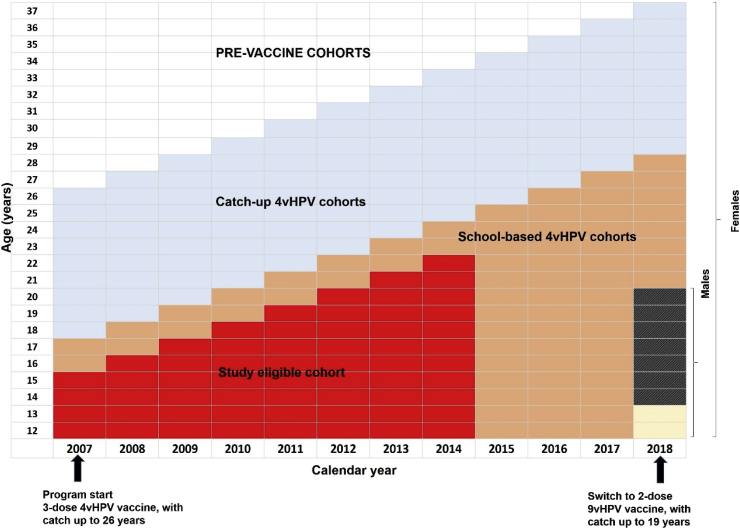
We linked registry data from all 8 jurisdictional cervical screening registers, with the national HPV vaccination register, death index and cancer registers for all Australian women aged 15 or under when eligible for vaccine who screened between April 2007 (when vaccination commenced) and 31 December 2014. We performed Cox proportional hazard regression, adjusted a priori for age, socioeconomic status, and area of residence, to estimate hazard ratios of histologically confirmed CIN2/CIN3/AIS/cancer.
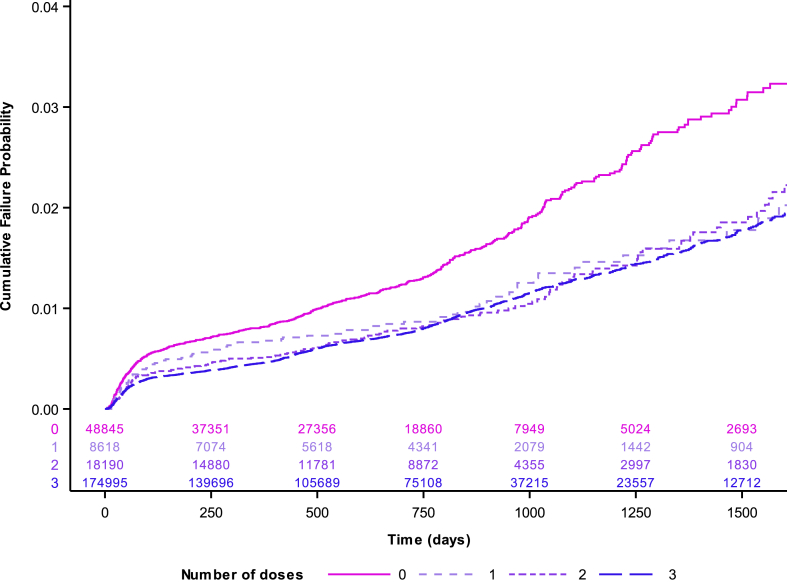
We included 250,648 women: 48,845 (19·5%) unvaccinated, 174,995 (69·8%) had received three doses, 18,190 (7·3%) two doses and 8,618 (3·4%) one dose. The adjusted hazard ratio was significantly lower for all dose groups compared to unvaccinated women (1 dose 0·65 (95%CI 0·52-0·81), 2 doses 0·61 (0·52-0·72) and 3 doses 0·59 (0·54-0·65).) With adjustment for age at vaccination amongst the vaccinated group, the adjusted hazard ratios for one dose and two dose recipients were comparable to three dose recipients (one dose 1.01 (95%CI 0.81-1.26), two doses 1.00 (0.85-1.17).) Multiple sensitivity analyses, including use of different dose assignment methods, produced consistent findings. Comparison with a historical cohort of age matched women showed that the result was not due to herd protection alone.
One dose had comparable effectiveness as two or three doses in preventing high-grade disease in a high coverage setting. These findings support the hypothesis that one dose vaccination may be a viable strategy when working towards the global elimination of cervical cancer.
预防性人乳头瘤病毒(HPV)疫苗按三剂方案接种时,在预防癌前宫颈病变方面非常有效。一些事后试验数据表明,一剂疫苗可预防HPV感染。如果一剂疫苗就能预防癌前宫颈病变,那么全球宫颈癌预防工作将得到极大推动。我们评估了四价HPV疫苗在澳大利亚接种后长达七年的时间里,按接种剂数对宫颈上皮内瘤变(CIN)2或3/原位腺癌(AIS)/癌症的预防效果。
我们将澳大利亚所有8个辖区的宫颈筛查登记处的登记数据,与国家HPV疫苗接种登记处、死亡索引和癌症登记处的数据相链接,这些数据涉及2007年4月(疫苗接种开始时)至2014年12月31日期间符合疫苗接种条件且年龄在15岁及以下的所有澳大利亚女性,她们均接受了宫颈筛查。我们进行了Cox比例风险回归分析,并对年龄、社会经济地位和居住地区进行了先验调整,以估计经组织学确诊的CIN2/CIN3/AIS/癌症的风险比。
我们纳入了250,648名女性:48,845名(19.5%)未接种疫苗,174,995名(69.8%)接种了三剂,18,190名(7.3%)接种了两剂,8,618名(3.4%)接种了一剂。与未接种疫苗的女性相比,所有接种剂量组的调整后风险比均显著降低(一剂0.65(95%置信区间0.52 - 0.81),两剂0.61(0.52 - 0.72),三剂0.59(0.54 - 0.65))。在接种疫苗组中对接种年龄进行调整后,一剂和两剂接种者的调整后风险比与三剂接种者相当(一剂1.01(95%置信区间0.81 - 1.26),两剂1.00(0.85 - 1.17))。多项敏感性分析,包括使用不同的剂量分配方法,得出了一致的结果。与年龄匹配的历史队列女性进行比较表明,结果并非仅归因于群体保护。
在高接种覆盖率的情况下,一剂疫苗在预防高级别疾病方面与两剂或三剂疫苗具有相当的效果。这些发现支持了这样一种假设,即在努力实现全球消除宫颈癌的过程中,一剂疫苗接种可能是一种可行的策略。