Epidemiology Unit, Azienda USL-IRCCS di Reggio Emilia, Reggio Emilia, Italy.
Clinical and Experimental Medicine PhD Program, University of Modena and Reggio Emilia, Modena, Italy.
PLoS One. 2019 Jul 22;14(7):e0219965. doi: 10.1371/journal.pone.0219965. eCollection 2019.
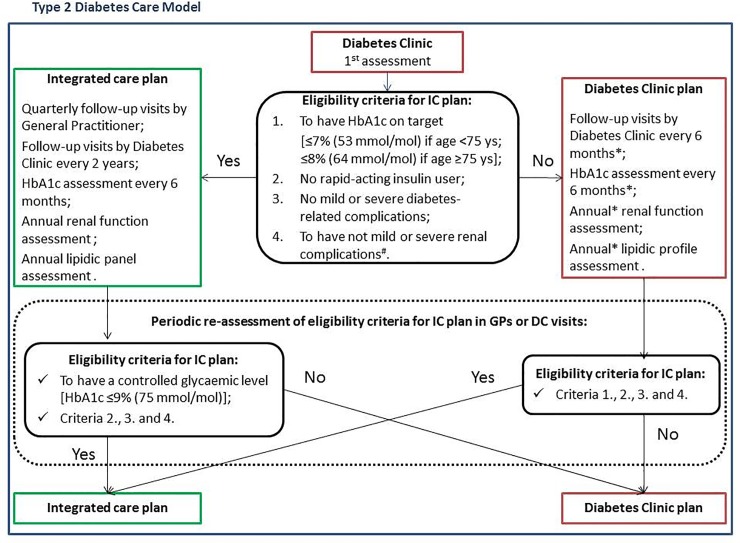
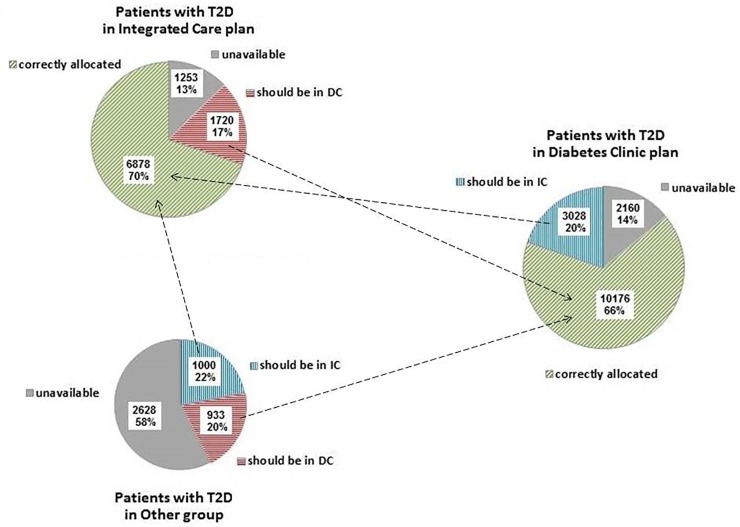
The study aims to describe the distribution of patients with type 2 diabetes (T2D) by care plan and to highlight determinants of underuse and overuse of integrated care (IC). This cross-sectional study included all T2D patients resident in Reggio Emilia on 31/12/2015 based on the population-based diabetes registry. Eligibility for IC requires good glycaemic control, no rapid insulin, no kidney failure and no diabetes complications. We calculated the proportion of IC underuse and overuse and adjusted prevalence estimate using multivariate logistic regression. Determinants were age, sex, citizenship, district of residence and time since diagnosis. Of 29,776 patients, 15,364 (51.6%) were in diabetes clinic plan, 9851 (33.1%) in IC plan and 4561 (15.3%) not in any care plan (i.e., in Other group). There were 10,906 (36.6%) patients eligible for IC, of whom 1000 in Other group. When we adjusted for all covariates and restricted the analysis to patients included in care plans, the proportion of those eligible for IC plan but cared for in diabetes clinic plan (i.e. underuse of IC) was 28% (n = 3028/9906; 95%CI 27-29). Similarly, the proportion of those not eligible for IC but cared for in IC plan (i.e. overuse of IC) was 11% (n = 1720/11,896; 95%CI 10-11).The main determinant of both IC underuse and overuse was the district of residence. Foreign status was associated with underuse (37%; 95%CI 33-43), while old age (≥80 years) with both underuse (36%; 95%CI 0.33-0.38) and overuse (23%; 95%CI 22-25). The criterion for suspension of IC plan most frequently found was renal failure, followed by hospitalization for diabetes-related complications. Patients are more often allocated to more specialized settings than not. Healthcare provider-related factors are the main determinants of inappropriate setting allocation.
本研究旨在描述按护理计划分类的 2 型糖尿病(T2D)患者分布,并突出整合护理(IC)利用不足和过度利用的决定因素。这项横断面研究基于人群糖尿病登记处,纳入了 2015 年 12 月 31 日居住在雷焦艾米利亚的所有 T2D 患者。IC 适用条件为血糖控制良好、无速效胰岛素、无肾功能衰竭和无糖尿病并发症。我们计算了 IC 利用不足和过度利用的比例,并使用多变量逻辑回归调整了患病率估计值。决定因素为年龄、性别、国籍、居住地区和诊断后时间。在 29776 名患者中,15364 名(51.6%)在糖尿病诊所计划中,9851 名(33.1%)在 IC 计划中,4561 名(15.3%)未在任何护理计划中(即其他组)。有 10906 名(36.6%)患者符合 IC 条件,其中 1000 名在其他组中。当我们调整所有协变量并将分析仅限于纳入护理计划的患者时,符合 IC 计划但在糖尿病诊所计划中接受治疗的患者比例(即 IC 利用不足)为 28%(n=3028/9906;95%CI 27-29)。同样,不符合 IC 条件但在 IC 计划中接受治疗的患者比例(即 IC 过度利用)为 11%(n=1720/11896;95%CI 10-11)。IC 利用不足和过度利用的主要决定因素是居住地区。外国公民身份与利用不足有关(37%;95%CI 33-43),而高龄(≥80 岁)与利用不足(36%;95%CI 0.33-0.38)和过度利用(23%;95%CI 22-25)有关。最常发现的 IC 计划暂停标准是肾功能衰竭,其次是糖尿病相关并发症住院治疗。患者通常被分配到更专门的环境中,而不是不分配。医疗保健提供者相关因素是不合理环境分配的主要决定因素。