Celgene Corporation, Summit, NJ, USA.
Celgene Corporation, Seattle, WA, USA.
Clin Pharmacokinet. 2020 Feb;59(2):217-227. doi: 10.1007/s40262-019-00804-x.
Durvalumab, a human monoclonal antibody targeting programmed cell death ligand 1, has been approved for urothelial carcinoma and stage III non-small cell lung cancer by the US Food and Drug Administration and is being evaluated in various malignancies. The objective of this study was to develop a population-pharmacokinetic model of durvalumab in patients with various hematologic malignancies and to investigate the effects of demographic and disease factors on the pharmacokinetics in this population.
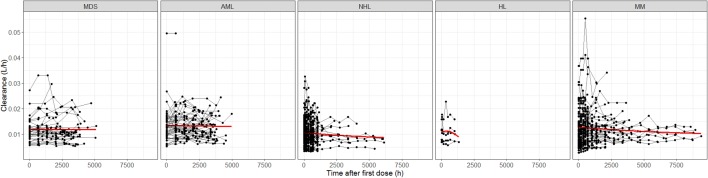
A total of 1812 concentrations from 267 patients with myelodysplastic syndromes, acute myeloid leukemia, multiple myeloma, non-Hodgkin lymphoma, or Hodgkin lymphoma were included in the analysis.
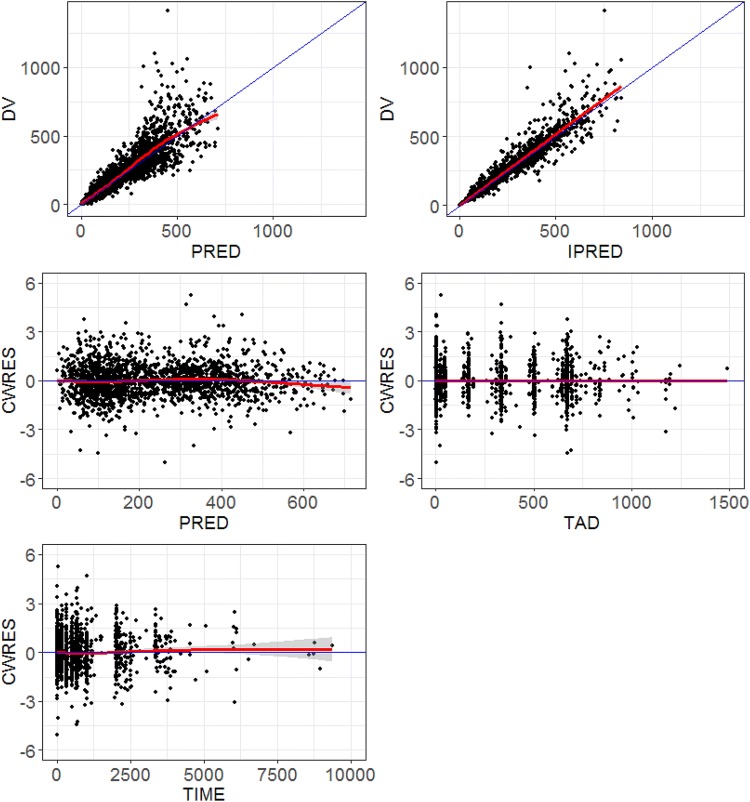
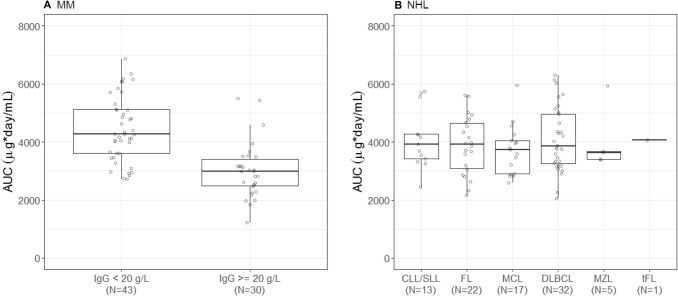
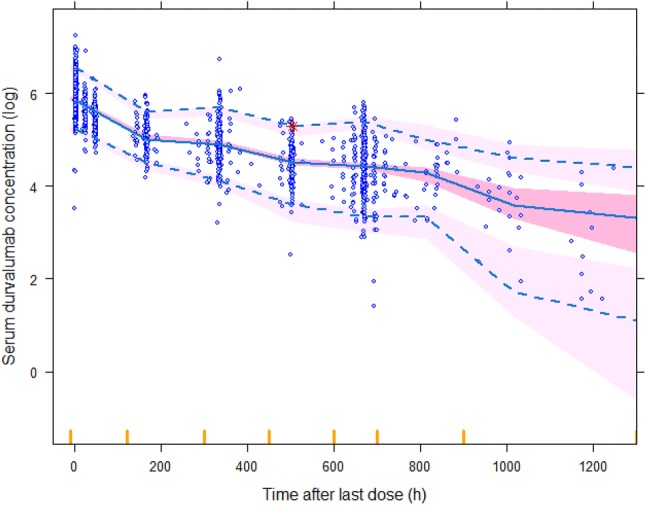
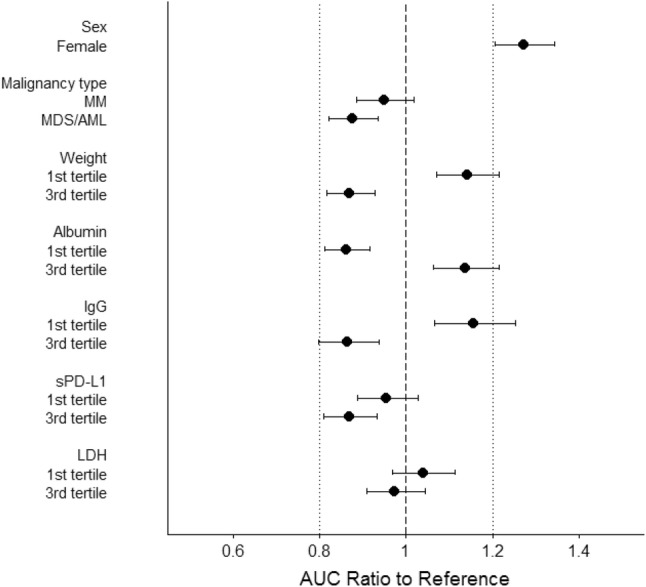
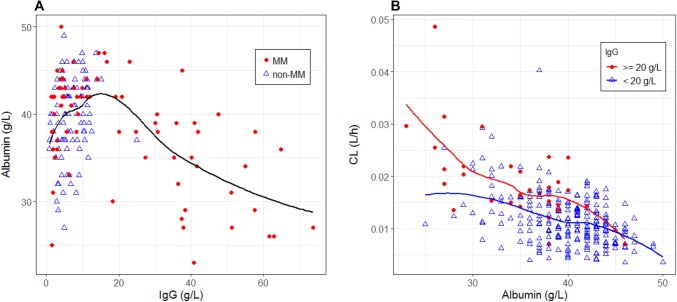
The pharmacokinetics of durvalumab was adequately described by a two-compartment model with first-order elimination. A decrease in durvalumab clearance over time was mainly explained by incorporation of time-dependent changes in albumin (in all patients) and immunoglobulin G (in patients with multiple myeloma) into the model. For multiple myeloma, patients with immunoglobulin G ≥ 20 g/L showed a 30% lower area under the concentration-time curve at cycle 1 compared with patients with immunoglobulin G < 20 g/L. The impact of any baseline covariates on durvalumab pharmacokinetics did not appear to be clinically relevant. The pharmacokinetics of durvalumab in hematologic malignancies was generally consistent with previously reported pharmacokinetics in solid tumors.
These results support the same dosing regimen (1500 mg every 4 weeks) for both solid tumors and hematologic malignancies from the perspective of adequate exposure. Additionally, total immunoglobulin G level could be a critical covariate for the pharmacokinetics of monoclonal antibodies in patients with multiple myeloma.
度伐鲁单抗是一种针对程序性死亡配体 1 的人源单克隆抗体,已被美国食品和药物管理局批准用于治疗尿路上皮癌和 III 期非小细胞肺癌,并正在各种恶性肿瘤中进行评估。本研究的目的是建立度伐鲁单抗在各种血液恶性肿瘤患者中的群体药代动力学模型,并探讨人口统计学和疾病因素对该人群药代动力学的影响。
共纳入 267 例骨髓增生异常综合征、急性髓系白血病、多发性骨髓瘤、非霍奇金淋巴瘤或霍奇金淋巴瘤患者的 1812 个浓度数据进行分析。
度伐鲁单抗的药代动力学通过具有一级消除的两室模型得到了很好的描述。度伐鲁单抗清除率随时间的下降主要归因于将白蛋白(所有患者)和免疫球蛋白 G(多发性骨髓瘤患者)的时间依赖性变化纳入模型。对于多发性骨髓瘤患者,与免疫球蛋白 G < 20 g/L 的患者相比,免疫球蛋白 G ≥ 20 g/L 的患者在第 1 周期的曲线下面积(AUC)降低了 30%。任何基线协变量对度伐鲁单抗药代动力学的影响似乎没有临床意义。血液恶性肿瘤中度伐鲁单抗的药代动力学与先前报道的实体瘤药代动力学基本一致。
从充分暴露的角度来看,这些结果支持在实体瘤和血液恶性肿瘤中使用相同的给药方案(1500 mg,每 4 周 1 次)。此外,总免疫球蛋白 G 水平可能是多发性骨髓瘤患者单克隆抗体药代动力学的关键协变量。