Department of Gastrointestinal Oncology, Key Laboratory of Carcinogenesis and Translational Research (Ministry of Education), Peking University Cancer Hospital & Institute, Beijing, China.
Genecast Precision Medicine Technology Institute, Beijing, China.
JAMA Netw Open. 2019 Jul 3;2(7):e197621. doi: 10.1001/jamanetworkopen.2019.7621.
There are a limited number of predictive biomarkers for hyperprogressive disease (HPD), which is induced by immune checkpoint blockade (ICB) therapy.
To evaluate the association of biomarkers in serum with the response to ICB therapy in patients with metastatic gastrointestinal tract cancer.
DESIGN, SETTING, AND PARTICIPANTS: Cohort study in which patients with metastatic gastrointestinal tract cancer treated with ICB were enrolled at the Department of Gastrointestinal Oncology, Peking University Cancer Hospital and Institute, Beijing, China, from August 1, 2015, to July 31, 2017, with the last follow-up date on January 1, 2018. Serum samples were collected at baseline and during the first visit to the clinic after starting treatment. Data analysis was conducted from January 16, 2018, to September 1, 2018.
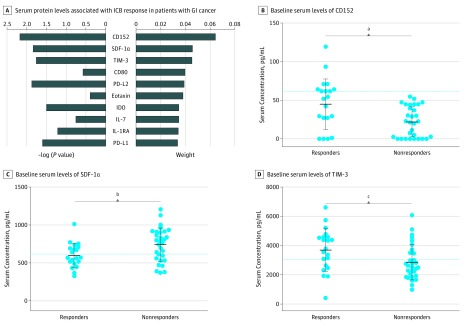
A total of 59 factors, including cytokines/chemokines, growth factors, and soluble checkpoint-related proteins in serum, were examined by multiplexed bead immunoassays.
Tree-based estimators were used to evaluate the importance of serum protein levels to ICB treatment response. Progression-free survival and overall survival analyses were conducted with the Kaplan-Meier method and log-rank test.
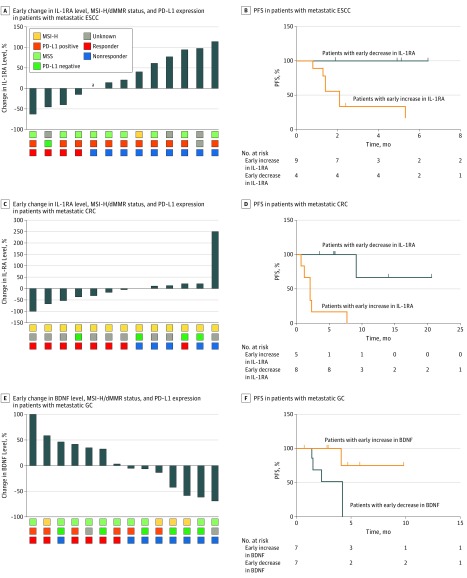
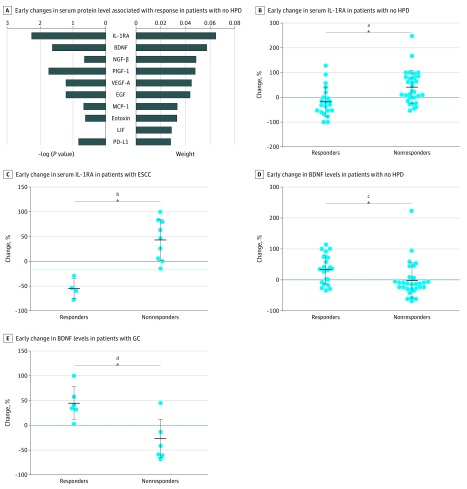
In total, 56 patients were examined. All patients with HPD (5 [8.9%]) had significantly lower mean (SD) levels of serum monocyte chemoattractant protein 1 than patients without HPD at baseline (53.4 [17.3] pg/mL vs 106.4 [48.4] pg/mL; P = .02). All patients with HPD were also identified by lower leukemia inhibitory factor levels (<13.28 pg/mL) and higher cluster of differentiation 152 levels (≥31.81 pg/mL). Among the remaining 51 patients, responders with esophageal squamous cell carcinoma (ESCC) or colorectal cancer (CRC) showed larger decreases in interleukin 1 receptor antagonist levels than nonresponders (ESCC: -55.02% [95% CI, -86.52% to -23.51%] vs 43.44% [95% CI, 11.93% to 74.96%]; P < .001; CRC: -35.82% [95% CI, -67.38% to -4.26%] vs 59.14% [95% CI, -72.34% to 190.6%]; P = .04). Responders with gastric cancer (GC) had larger increases in brain-derived neurotrophic factor levels than nonresponders (44.77% [95% CI, 10.76% to 78.79%] vs -26.2% [95% CI, -58.53% to 6.12%]; P = .003). Furthermore, early decreases in serum interleukin 1 receptor antagonist in patients with metastatic ESCC and CRC were associated with longer progression-free survival (ESCC: not reached vs 2.1 months; hazard ratio, 0.19; 95% CI, 0.04 to 0.95; P = .04; CRC: not reached vs 2.1 months; hazard ratio, 0.06; 95% CI, 0.01 to 0.38; P < .001). Early increases in brain-derived neurotrophic factor levels in patients with metastatic GC were associated with longer progression-free survival (not reached vs 4.2 months; hazard ratio, 0.15; 95% CI, 0.03 to 0.84; P = .03).
In this study, baseline serum levels of monocyte chemoattractant protein 1, leukemia inhibitory factor, and cluster of differentiation 152 were associated with hyperprogressive metastatic gastrointestinal cancer among patients receiving ICB. An early decrease in serum interleukin 1 receptor antagonist levels in patients with metastatic ESCC or CRC and an early increase in serum brain-derived neurotrophic factor levels in patients with metastatic GC were better able to identify who would respond to ICB compared with microsatellite stability status or programmed cell death ligand 1 expression.
目前用于预测免疫检查点阻断(ICB)治疗诱导的 hyperprogressive disease(HPD)的预测生物标志物数量有限。
评估转移性胃肠道癌患者的 ICB 治疗反应与血清生物标志物之间的关联。
设计、地点和参与者:本队列研究纳入了 2015 年 8 月 1 日至 2017 年 7 月 31 日在北京北京大学肿瘤医院胃肠肿瘤内科接受 ICB 治疗的转移性胃肠道癌患者,最后随访日期为 2018 年 1 月 1 日。在开始治疗后的首次就诊时采集基线和血清样本。数据分析于 2018 年 1 月 16 日至 2018 年 9 月 1 日进行。
通过多重珠免疫分析检测血清中的细胞因子/趋化因子、生长因子和可溶性检查点相关蛋白等共 59 个因素。
采用基于树的估计器评估血清蛋白水平对 ICB 治疗反应的重要性。使用 Kaplan-Meier 方法和对数秩检验进行无进展生存期和总生存期分析。
共纳入 56 例患者。所有 HPD(5 [8.9%])患者的基线血清单核细胞趋化蛋白 1 水平显著低于非 HPD 患者(53.4 [17.3] pg/mL 比 106.4 [48.4] pg/mL;P = 0.02)。所有 HPD 患者的白血病抑制因子水平也较低(<13.28 pg/mL),CD152 水平较高(≥31.81 pg/mL)。在其余 51 例患者中,食管鳞状细胞癌(ESCC)或结直肠癌(CRC)的应答者与非应答者相比,白细胞介素 1 受体拮抗剂水平下降幅度更大(ESCC:-55.02%[95%CI,-86.52%至-23.51%]比 43.44%[95%CI,11.93%至 74.96%];P<0.001;CRC:-35.82%[95%CI,-67.38%至-4.26%]比 59.14%[95%CI,-72.34%至 190.6%];P = 0.04)。胃癌(GC)的应答者与非应答者相比,脑源性神经营养因子水平升高幅度更大(44.77%[95%CI,10.76%至 78.79%]比-26.2%[95%CI,-58.53%至 6.12%];P = 0.003)。此外,转移性 ESCC 和 CRC 患者血清白细胞介素 1 受体拮抗剂早期下降与无进展生存期延长相关(ESCC:未达到与 2.1 个月;风险比,0.19;95%CI,0.04 至 0.95;P = 0.04;CRC:未达到与 2.1 个月;风险比,0.06;95%CI,0.01 至 0.38;P<0.001)。转移性 GC 患者脑源性神经营养因子水平早期升高与无进展生存期延长相关(未达到与 4.2 个月;风险比,0.15;95%CI,0.03 至 0.84;P = 0.03)。
在这项研究中,基线时血清单核细胞趋化蛋白 1、白血病抑制因子和 CD152 水平与接受 ICB 治疗的转移性胃肠道癌患者的 HPD 相关。转移性 ESCC 或 CRC 患者血清白细胞介素 1 受体拮抗剂水平早期下降,转移性 GC 患者血清脑源性神经营养因子水平早期升高,与微卫星不稳定性状态或程序性死亡配体 1 表达相比,更能识别出对 ICB 有反应的患者。