Patel Neil, Powell Arfon G, Wheat Jenni R, Brown Christopher, Appadurai Ian R, Davies Richard G, Bailey Damian M, Lewis Wyn G
Department of General Surgery, University Hospital of Wales, Cardiff, United Kingdom.
Division of Cancer and Genetics, Cardiff University School of Medicine, Heath Park, Cardiff, United Kingdom.
Physiol Rep. 2019 Jul;7(14):e14174. doi: 10.14814/phy2.14174.
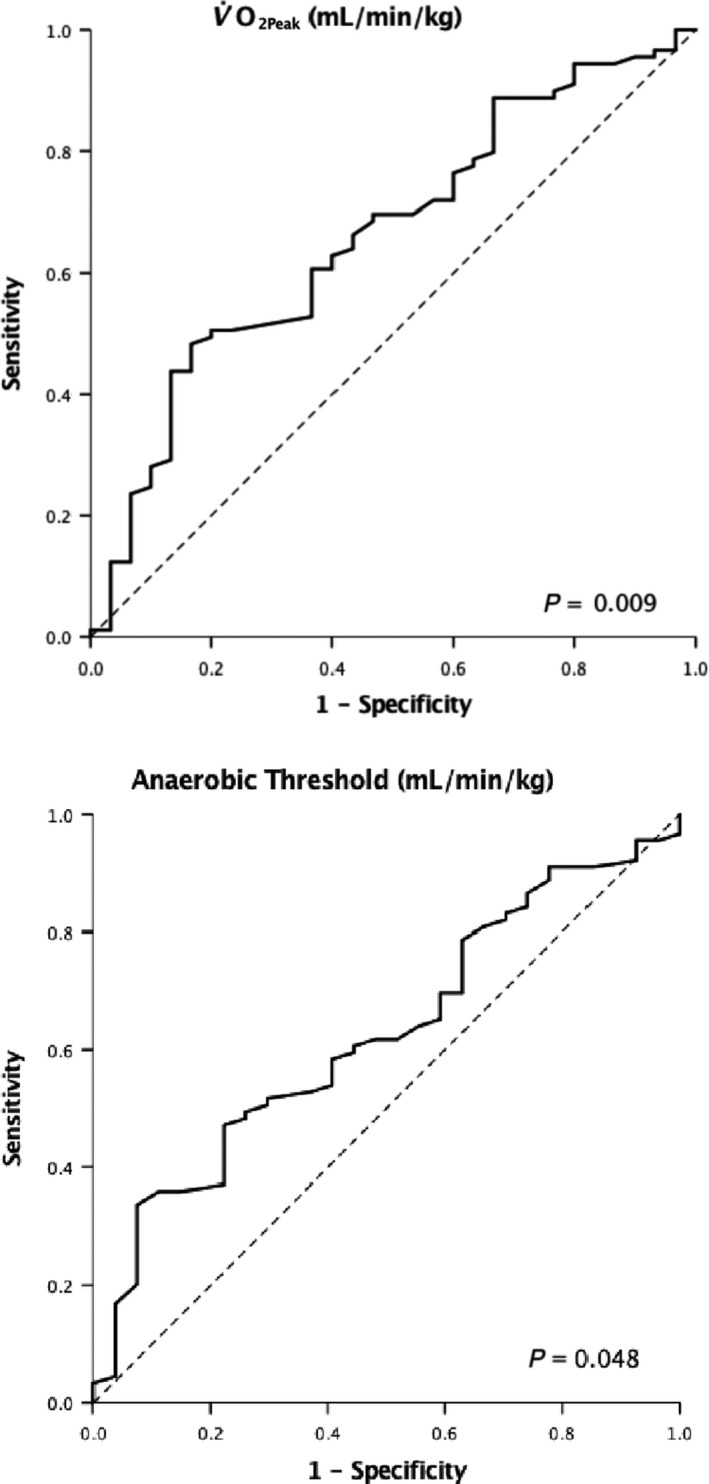
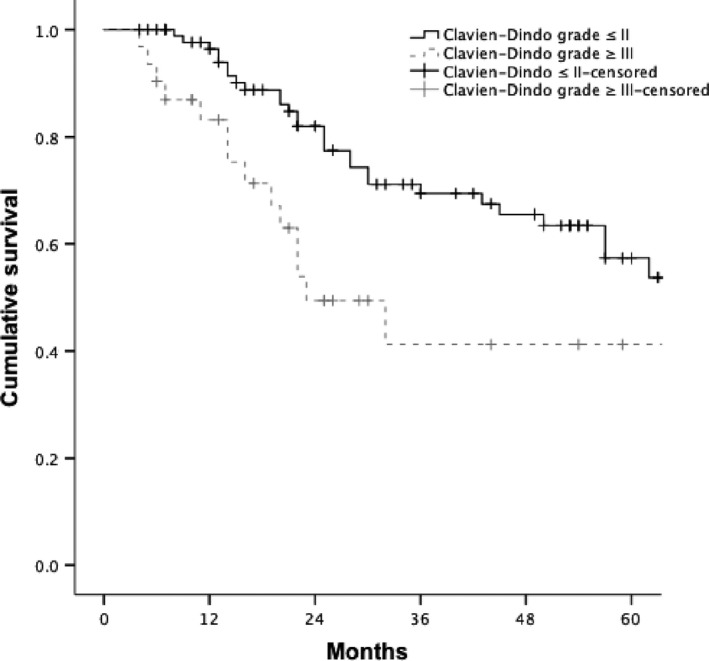
Surgery for radical treatment of esophageal cancer (EC) carries significant inherent risk. The objective identification of patients who are at high risk of complications is of importance. In this study the prognostic value of cardiopulmonary fitness variables (CPF) derived from cardiopulmonary exercise testing (CPET) was assessed in patients undergoing potentially curative surgery for EC within an enhanced recovery program. OC patients underwent preoperative CPET using automated breath-by-breath respiratory gas analysis, with measurements taken during a ramped exercise test on a bicycle. The prognostic value of , Anaerobic Threshold (AT) and VE/VCO derived from CPET were studied in relation to post-operative morbidity, which was collected prospectively, and overall survival. Consecutive 120 patients were included for analysis (median age 65 years, 100 male, 75 neoadjuvant therapy). Median AT in the cohort developing major morbidity (Clavien-Dindo classification >2) was 10.4 mL/kg/min compared with 11.3 mL/kg/min with no major morbidity (P = 0.048). Median in the cohort developing major morbidity was 17.0 mL/kg/min compared with 18.7 mL/kg/min in the cohort (P = 0.009). optimum cut-off was 17.0 mL/kg/min (sensitivity 70%, specificity 53%) and for AT was 10.5 mL/kg/min (sensitivity 60%, specificity 44%). Multivariable analysis revealed to be the only independent factor to predict major morbidity (OR 0.85, 95% CI 0.75-0.97, P = 0.018). Cumulative survival was associated with operative morbidity severity (χ = 4.892, df = 1, P = 0.027). These results indicate that as derived from CPET is a significant predictor of major morbidity after oesophagectomy highlighting the physiological importance of cardiopulmonary fitness.
食管癌(EC)根治性手术具有显著的固有风险。客观识别并发症高风险患者至关重要。在本研究中,对强化康复计划下接受潜在根治性食管癌手术患者的心肺运动试验(CPET)得出的心肺功能变量(CPF)的预后价值进行了评估。食管癌患者使用自动逐次呼吸呼吸气体分析进行术前CPET,测量在自行车递增运动试验期间进行。研究了CPET得出的[具体变量未给出]、无氧阈值(AT)和VE/VCO与术后发病率(前瞻性收集)及总生存期的预后价值。连续纳入120例患者进行分析(中位年龄65岁,男性100例,75例接受新辅助治疗)。发生严重并发症(Clavien-Dindo分类>2)队列的中位AT为10.4 mL/kg/min,无严重并发症队列的中位AT为11.3 mL/kg/min(P = 0.048)。发生严重并发症队列的中位[具体变量未给出]为17.0 mL/kg/min,另一队列的中位[具体变量未给出]为18.7 mL/kg/min(P = 0.009)。[具体变量未给出]的最佳截断值为17.0 mL/kg/min(敏感性70%,特异性53%),AT的最佳截断值为10.5 mL/kg/min(敏感性60%,特异性44%)。多变量分析显示[具体变量未给出]是预测严重并发症的唯一独立因素(OR 0.85,95%CI 0.75 - 0.97,P = 0.018)。累积生存率与手术并发症严重程度相关(χ² = 4.892,df = 1,P = 0.027)。这些结果表明,CPET得出的[具体变量未给出]是食管切除术后严重并发症的重要预测指标,突出了心肺功能的生理重要性。