Centre for Tropical Medicine and Global Health, Nuffield Department of Medicine, University of Oxford, United Kingdom.
London Centre for Neglected Tropical Disease Research, Imperial College London, United Kingdom.
Clin Infect Dis. 2020 Jun 10;70(12):2561-2567. doi: 10.1093/cid/ciz671.
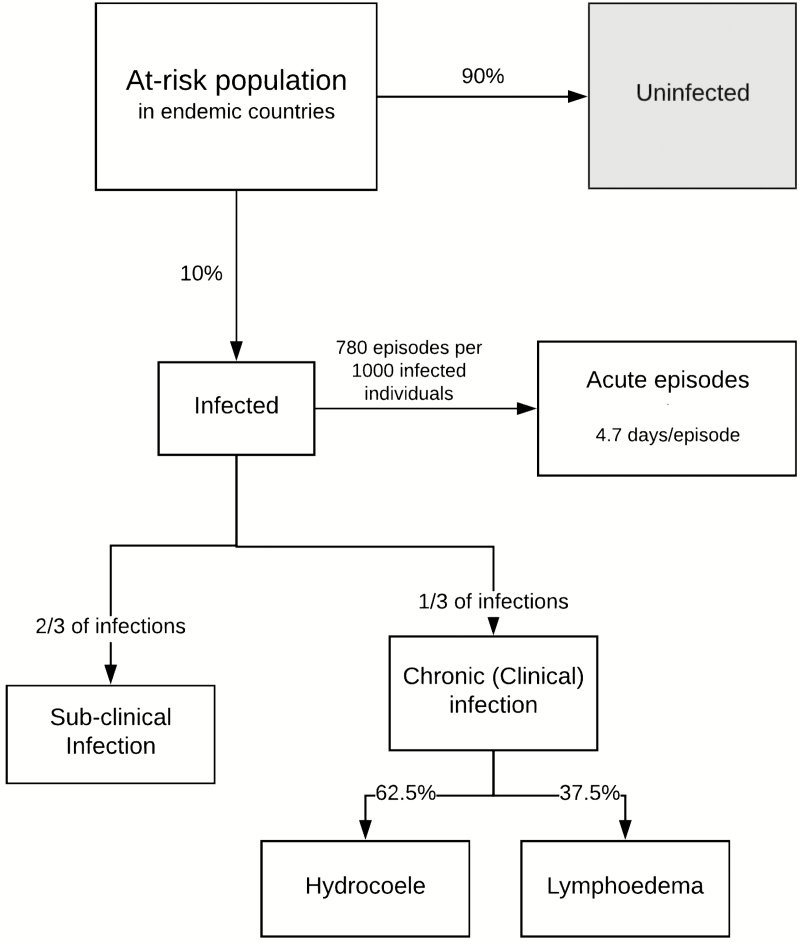
The Global Programme to Eliminate Lymphatic Filariasis (GPELF) was launched in 2000 with the goal of eliminating lymphatic filariasis (LF) as a public health problem by 2020. Despite considerable progress, the current prevalence is around 60% of the 2000 figure, with the deadline looming a year away. Consequently, there is a continued need for investment in both the mass drug administration (MDA) and morbidity management programs, and this paper aims to demonstrate that need by estimating the health and economic burdens of LF prior to MDA programs starting in GPELF areas.
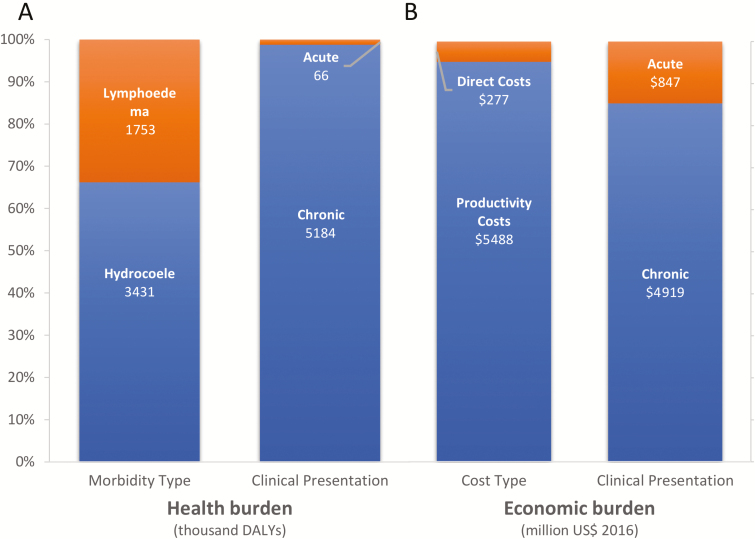
A previously developed model was used to estimate the numbers of individuals infected and individuals with symptomatic disease, along with the attributable number of disability-adjusted life years (DALYs). The economic burden was calculated by quantifying the costs incurred by the health-care system in managing clinical cases, the patients' out-of-pocket costs, and their productivity costs.
Prior to the MDA program, approximately 129 million people were infected with LF, of which 43 million had clinical disease, corresponding to a DALY burden of 5.25 million. The average annual economic burden per chronic case was US $115, the majority of which resulted from productivity costs. The total economic burden of LF was estimated at US $5.8 billion annually.
These results demonstrate the magnitude of the LF burden and highlight the continued need to support the GPELF. Patients with clinical disease bore the majority of the economic burden, but will not benefit much from the current MDA program, which is aimed at reducing transmission. This assessment further highlights the need to scale up morbidity management programs.
全球消灭淋巴丝虫病规划(GPELF)于 2000 年启动,目标是到 2020 年消除淋巴丝虫病(LF)这一公共卫生问题。尽管取得了相当大的进展,但目前的流行率仍约为 2000 年的 60%,距离截止日期还有一年。因此,仍需要继续投资于大规模药物治疗(MDA)和发病率管理方案,本文旨在通过在 GPELF 地区开始 MDA 项目之前,估计 LF 的健康和经济负担,来证明这一需求。
使用之前开发的模型来估计感染人数和有症状疾病人数,以及归因于残疾调整生命年(DALY)的人数。通过量化卫生保健系统在管理临床病例、患者自付费用和生产力成本方面所产生的成本,计算经济负担。
在 MDA 项目开始之前,约有 1.29 亿人感染 LF,其中 4300 万人患有临床疾病,对应的 DALY 负担为 525 万。慢性病例的平均年经济负担为 115 美元,其中大部分来自生产力成本。LF 的总经济负担估计为每年 58 亿美元。
这些结果表明 LF 负担的规模,并强调继续支持 GPELF 的必要性。患有临床疾病的患者承担了大部分经济负担,但他们不会从当前旨在减少传播的 MDA 项目中受益太多。这一评估进一步强调了扩大发病率管理方案的必要性。