Department of Gastroenterology, Hospital Universitari Mutua Terrassa, Plaza Dr Robert 5, 08221, Terrassa, Barcelona, Spain.
Centro de Investigación Biomédica en Red de enfermedades hepáticas y digestivas (CIBERehd), Instituto Salud Carlos III, Madrid, Spain.
BMC Cancer. 2019 Jul 25;19(1):734. doi: 10.1186/s12885-019-5926-4.
Fast-track colonoscopy to detect patients with colorectal cancer based on high-risk symptoms is associated with low sensitivity and specificity. The aim was to derive a predictive score of advanced colonic neoplasia in symptomatic patients in fast-track programs.
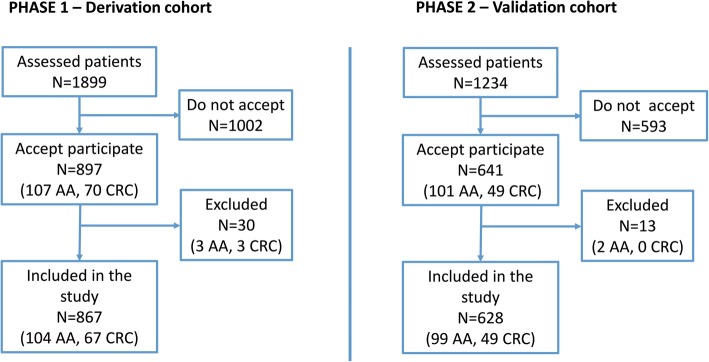
All patients referred for fast-track colonoscopy were evaluated. Faecal immunological haemoglobin test (3 samples; positive> 4 μg Hb/g), and a survey to register clinical variables of interest were performed. Colorectal cancer and advanced adenoma were considered as advanced colonic neoplasia. A sample size of 600 and 500 individuals were calculated for each phase 1 and phase 2 of the study, respectively (Phase 1, derivation and Phase 2, validation cohort). A Bayesian logistic regression analysis was used to derive a predictive score.
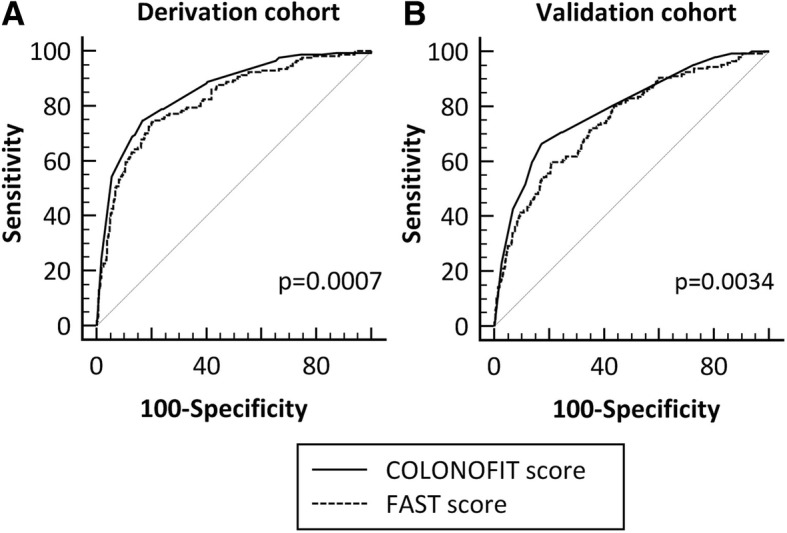
1495 patients were included. Age (OR, 21), maximum faecal-Hb value (OR, 2.3), and number of positive samples (OR, 28) presented the highest ORs predictive of advanced colonic neoplasia. The additional significant predictive variables adjusted for age and faecal-Hb variables in Phase 1 were previous colonoscopy (last 5 years) and smoking (no, ex/active). With these variables a predictive score of advanced colonic neoplasia was derived. Applied to Phase 2, patients with a Score > 20 had an advanced colonic neoplasia probability of 66% (colorectal cancer, 32%), while those with a Score ≤ 10, a probability of 10% (colorectal cancer, 1%). Prioritizing patients with Score > 10, 49.4% of patients would be referred for fast-track colonoscopy, diagnosing 98.3% of colorectal cancers and 77% of advanced adenomas.
A scoring system was derived and validated to prioritize fast-track colonoscopies according to risk, which was efficient, simple, and robust.
基于高危症状对结直肠癌患者进行快速通道结肠镜检查的敏感性和特异性较低。目的是为快速通道计划中的有症状患者建立一种预测高级结肠肿瘤的评分系统。
评估所有因快速通道结肠镜检查而就诊的患者。进行粪便免疫血红蛋白试验(3 个样本;阳性>4μg Hb/g),并进行登记感兴趣的临床变量的调查。结直肠癌和高级腺瘤被认为是高级结肠肿瘤。分别计算了每个研究阶段 1 和阶段 2 的样本量为 600 和 500 例(阶段 1,推导;阶段 2,验证队列)。使用贝叶斯逻辑回归分析来推导预测评分。
共纳入 1495 例患者。年龄(OR,21)、最大粪便-Hb 值(OR,2.3)和阳性样本数量(OR,28)是预测高级结肠肿瘤的最高 OR。在阶段 1 中,对年龄和粪便-Hb 变量进行调整后,另外两个具有预测价值的重要变量是既往结肠镜检查(过去 5 年)和吸烟(无、曾经/现在)。使用这些变量推导了高级结肠肿瘤的预测评分。在阶段 2 中应用该评分,评分>20 的患者高级结肠肿瘤的概率为 66%(结直肠癌,32%),而评分≤10 的患者概率为 10%(结直肠癌,1%)。优先考虑评分>10 的患者,将 49.4%的患者转诊进行快速通道结肠镜检查,诊断出 98.3%的结直肠癌和 77%的高级腺瘤。
建立并验证了一种评分系统,以根据风险对快速通道结肠镜检查进行优先排序,该系统高效、简单且稳健。