Department of Internal Medicine, Gastroenterology and Hepatology Unit, Catholic University of Health and Allied Sciences, P.O. Box 1464, Bugando, Mwanza, Tanzania.
Tropenmedizin, Missionsärztliche Klinik, Salvatorstr. 7, 97074 Würzburg, Germany.
Can J Gastroenterol Hepatol. 2019 Jul 1;2019:8481375. doi: 10.1155/2019/8481375. eCollection 2019.
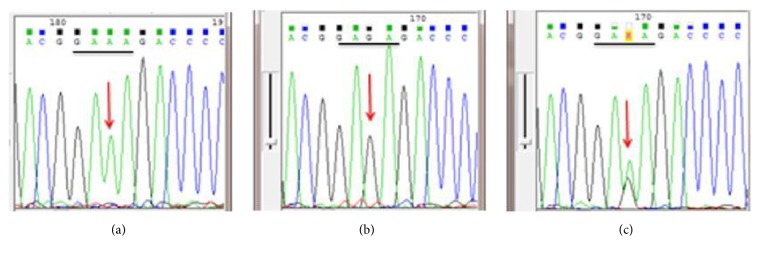
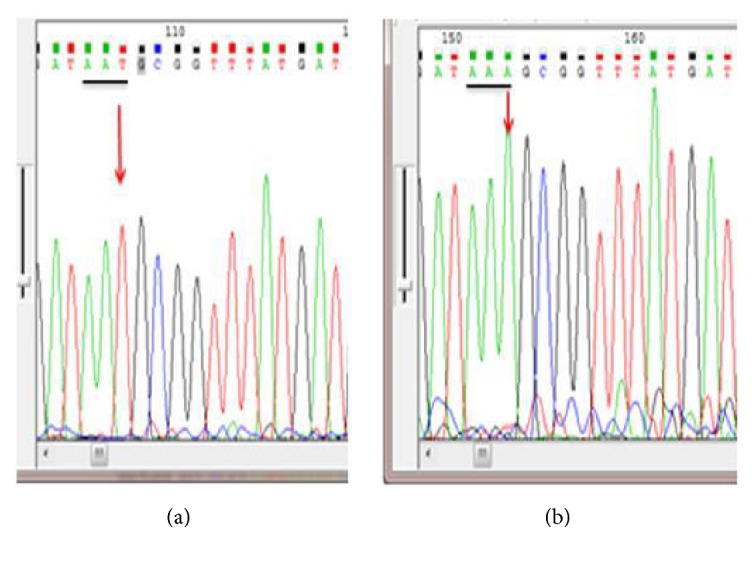
() isolates resistant to clarithromycin and quinolones are increasing worldwide. Data regarding the magnitude of resistance are limited in developing countries. Here, we report the prevalence of mutations conferring resistance to clarithromycin and fluoroquinolones among dyspeptic patients attending a tertiary hospital, Tanzania. Between August 2014 and August 2016, patients undergoing upper gastrointestinal endoscopy at the Bugando Medical Centre were enrolled. Biopsies were taken for polymerase chain reaction (PCR) and sequencing to detect mutations conferring resistance to clarithromycin and fluoroquinolones. A total of 208 nonrepetitive biopsies were examined of which 188 (90.4%) tested positive for specific 23S rRNA PCR. Clarithromycin resistance mutations were detected in 54/188 (28.7%) of patients tested. The most frequently detected mutation was A2143G (30) followed by A2142G (20). Out of 131 nonrepetitive biopsies tested for fluoroquinolones resistance mutations, 77/131 (58.8%) were positive, with N87I (20) mutation being the most frequently detected mutation followed by A92T mutation which was detected in 16 samples. A significant proportion of dyspeptic patients attending tertiary hospital in Tanzania are infected with strains harbouring clarithromycin or fluoroquinolones resistance mutations. Detection of more than 50% of strains with fluoroquinolones resistance mutations makes the second line treatment questionable in our setting. There is a need of surveillance of resistance patterns in Tanzania to provide data that can guide empirical treatment to reduce associated morbidity of infections. The correlation between A92T fluoroquinolone mutation and phenotypic resistance requires further investigations.
()对克拉霉素和喹诺酮类药物的耐药菌株在全球范围内不断增加。发展中国家关于耐药程度的数据有限。在这里,我们报告了坦桑尼亚一家三级医院消化不良患者对克拉霉素和氟喹诺酮类药物耐药的突变率。2014 年 8 月至 2016 年 8 月,布甘达医学中心接受上消化道内镜检查的患者被纳入研究。采集活检标本进行聚合酶链反应(PCR)和测序,以检测对克拉霉素和氟喹诺酮类药物耐药的突变。共检查了 208 份非重复活检标本,其中 188 份(90.4%)对特定 23S rRNA PCR 呈阳性。在接受检测的 188 名患者中,有 54 名(28.7%)检测到克拉霉素耐药突变。最常见的突变是 A2143G(30 例),其次是 A2142G(20 例)。在 131 份非重复活检标本中,有 77 份(58.8%)检测到氟喹诺酮类药物耐药突变,其中 N87I(20 例)突变最常见,其次是 A92T 突变,在 16 份样本中检测到。坦桑尼亚一家三级医院就诊的消化不良患者中,相当一部分感染了携带克拉霉素或氟喹诺酮类药物耐药突变的菌株。在我们的研究中,超过 50%的菌株对氟喹诺酮类药物耐药,这使得二线治疗受到质疑。有必要对坦桑尼亚的耐药模式进行监测,以提供数据,指导经验性治疗,减少相关感染的发病率。氟喹诺酮类药物突变与表型耐药之间的相关性需要进一步研究。