Calvaruso Luca, Naticchia Alessandro, Ferraro Pietro Manuel, Vischini Gisella, Costanzi Stefano
U.O.C. Nefrologia, Fondazione Policlinico Universitario A. Gemelli IRCCS, Rome, Italy.
Università Cattolica del Sacro Cuore, Rome, Italy.
Case Rep Nephrol. 2019 Jul 9;2019:9264824. doi: 10.1155/2019/9264824. eCollection 2019.
Atypical hemolytic uremic syndrome (aHUS) is characterized by microangiopathic hemolytic anemia, thrombocytopenia, and renal failure. Mutations in CFI gene coding for complement regulation factors and in THBD gene coding for endothelial cell receptor thrombomodulin could predispose to the disease and hypertension can trigger the onset.
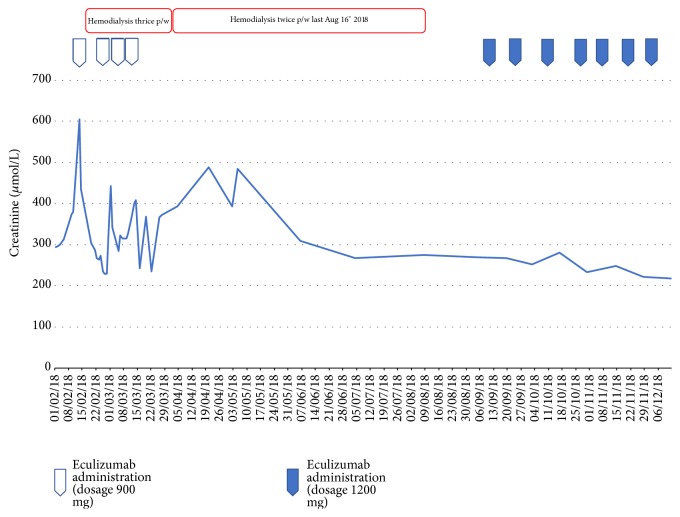
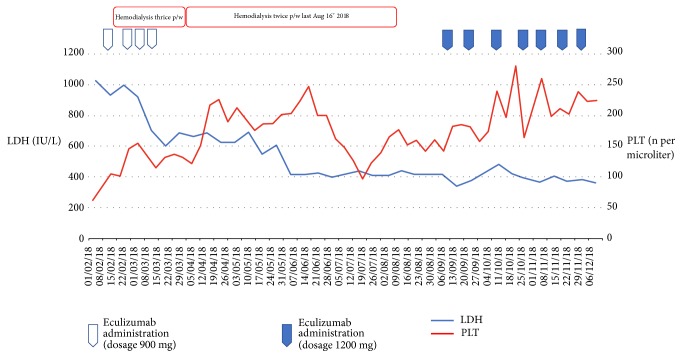
A 51-year-old female patient who had received kidney transplant eighteen years ago presented with hypertensive peak and hemolysis pattern. Normal ADAMTS13 levels as well as negative culture and serology for Shiga-toxin excluded, respectively, thrombotic thrombocytopenic purpura (TTP) and typical HUS caused by Shiga toxin-producing (STEC-HUS). In suspicion of aHUS, we administered eculizumab and hemodialysis sessions were started as the patient showed severe renal failure. After an initial response, the patient developed cerebral hemorrhage. After last eculizumab administration, according to hematological parameters, an unsatisfactory response was observed: given the worsening clinical scenario, we withdrew eculizumab. Pathogenic mutations in CFI and THBD genes were found. After eculizumab reinitiation, looking at hemolysis indexes, we observed a suboptimal response as well as an otherwise adequate renal one: renal graft function was recovered despite persistence of hemolysis signs, after 6 months on regular dialysis.
For the first time, we report an aHUS case in which a peculiar combination of mutations in CFI and THBD is found. We describe the importance of continuing eculizumab despite deterioration of patient's clinical conditions.
非典型溶血性尿毒症综合征(aHUS)的特征为微血管病性溶血性贫血、血小板减少和肾衰竭。编码补体调节因子的CFI基因及编码内皮细胞受体血栓调节蛋白的THBD基因发生突变可能易患该病,且高血压可触发其发病。
一名51岁女性患者,18年前接受了肾移植,出现高血压峰值和溶血模式。正常的ADAMTS13水平以及针对志贺毒素的培养和血清学阴性分别排除了血栓性血小板减少性紫癜(TTP)和由产志贺毒素大肠杆菌(STEC-HUS)引起的典型HUS。怀疑为aHUS,我们给予了依库珠单抗,并因患者出现严重肾衰竭而开始进行血液透析治疗。在最初有反应后,患者发生了脑出血。在最后一次给予依库珠单抗后,根据血液学参数观察到反应不理想:鉴于临床情况恶化,我们停用了依库珠单抗。发现CFI和THBD基因存在致病突变。重新开始使用依库珠单抗后,观察溶血指标,我们发现反应欠佳,但肾脏反应尚可:在定期透析6个月后,尽管溶血迹象持续存在,但肾移植功能恢复。
我们首次报告了一例发现CFI和THBD基因存在特殊突变组合的aHUS病例。我们描述了尽管患者临床状况恶化但仍继续使用依库珠单抗的重要性。