Schrijver Lieske H, Olsson Håkan, Phillips Kelly-Anne, Terry Mary Beth, Goldgar David E, Kast Karin, Engel Christoph, Mooij Thea M, Adlard Julian, Barrowdale Daniel, Davidson Rosemarie, Eeles Ros, Ellis Steve, Evans D Gareth, Frost Debra, Izatt Louise, Porteous Mary E, Side Lucy E, Walker Lisa, Berthet Pascaline, Bonadona Valérie, Leroux Dominique, Mouret-Fourme Emmanuelle, Venat-Bouvet Laurence, Buys Saundra S, Southey Melissa C, John Esther M, Chung Wendy K, Daly Mary B, Bane Anita, van Asperen Christi J, Gómez Garcia Encarna B, Mourits Marian J E, van Os Theo A M, Roos-Blom Marie-José, Friedlander Michael L, McLachlan Sue-Anne, Singer Christian F, Tan Yen Y, Foretova Lenka, Navratilova Marie, Gerdes Anne-Marie, Caldes Trinidad, Simard Jacques, Olah Edith, Jakubowska Anna, Arver Brita, Osorio Ana, Noguès Catherine, Andrieu Nadine, Easton Douglas F, van Leeuwen Flora E, Hopper John L, Milne Roger L, Antoniou Antonis C, Rookus Matti A
Department of Epidemiology, Netherlands Cancer Institute, Amsterdam, the Netherlands.
Department of Oncology, Lund University Hospital.
JNCI Cancer Spectr. 2018 Jun 28;2(2):pky023. doi: 10.1093/jncics/pky023. eCollection 2018 Apr.
For BRCA1 and BRCA2 mutation carriers, the association between oral contraceptive preparation (OCP) use and breast cancer (BC) risk is still unclear.
Breast camcer risk associations were estimated from OCP data on 6030 BRCA1 and 3809 BRCA2 mutation carriers using age-dependent Cox regression, stratified by study and birth cohort. Prospective, left-truncated retrospective and full-cohort retrospective analyses were performed.
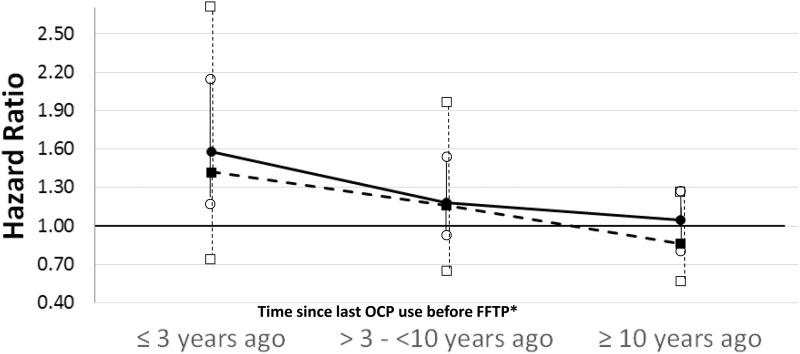
For BRCA1 mutation carriers, OCP use was not associated with BC risk in prospective analyses (hazard ratio [HR] = 1.08, 95% confidence interval [CI] = 0.75 to 1.56), but in the left-truncated and full-cohort retrospective analyses, risks were increased by 26% (95% CI = 6% to 51%) and 39% (95% CI = 23% to 58%), respectively. For BRCA2 mutation carriers, OCP use was associated with BC risk in prospective analyses (HR = 1.75, 95% CI = 1.03 to 2.97), but retrospective analyses were inconsistent (left-truncated: HR = 1.06, 95% CI = 0.85 to 1.33; full cohort: HR = 1.52, 95% CI = 1.28 to 1.81). There was evidence of increasing risk with duration of use, especially before the first full-term pregnancy (BRCA1: both retrospective analyses, < .001 and = .001, respectively; BRCA2: full retrospective analysis, = .002).
Prospective analyses did not show that past use of OCP is associated with an increased BC risk for BRCA1 mutation carriers in young middle-aged women (40-50 years). For BRCA2 mutation carriers, a causal association is also not likely at those ages. Findings between retrospective and prospective analyses were inconsistent and could be due to survival bias or a true association for younger women who were underrepresented in the prospective cohort. Given the uncertain safety of long-term OCP use for BRCA1/2 mutation carriers, indications other than contraception should be avoided and nonhormonal contraceptive methods should be discussed.
对于携带BRCA1和BRCA2基因突变的女性,口服避孕药(OCP)的使用与乳腺癌(BC)风险之间的关联仍不明确。
利用年龄依赖性Cox回归模型,根据6030名携带BRCA1基因突变者和3809名携带BRCA2基因突变者的口服避孕药数据,对乳腺癌风险关联进行评估,并按研究和出生队列进行分层。进行了前瞻性、左截断回顾性和全队列回顾性分析。
对于携带BRCA1基因突变的女性,在前瞻性分析中,口服避孕药的使用与乳腺癌风险无关(风险比[HR]=1.08,95%置信区间[CI]=0.75至1.56),但在左截断和全队列回顾性分析中,风险分别增加了26%(95%CI=6%至51%)和39%(95%CI=23%至58%)。对于携带BRCA2基因突变的女性,在前瞻性分析中,口服避孕药的使用与乳腺癌风险相关(HR=1.75,95%CI=1.03至2.97),但回顾性分析结果不一致(左截断:HR=1.06,95%CI=0.85至1.33;全队列:HR=1.52,95%CI=1.28至1.81)。有证据表明,随着使用时间的延长,风险增加,尤其是在首次足月妊娠之前(BRCA1:两项回顾性分析,分别为P<0.001和P=0.001;BRCA2:全回顾性分析,P=0.002)。
前瞻性分析未显示过去使用口服避孕药会增加年轻中年女性(40 - 50岁)携带BRCA1基因突变者患乳腺癌的风险。对于携带BRCA2基因突变的女性,在这些年龄段也不太可能存在因果关联。回顾性和前瞻性分析结果不一致,可能是由于生存偏差,或者是因为在前瞻性队列中代表性不足的年轻女性存在真正的关联。鉴于长期使用口服避孕药对携带BRCA1/2基因突变者的安全性不确定,应避免将其用于避孕以外的其他用途,并应讨论非激素避孕方法。