Flugelman Anath A, Stein Nili, Segol Ori, Lavi Idit, Keinan-Boker Lital
Department of Community Medicine and Epidemiology, Lady Davis Carmel Medical Center, Haifa, Israel.
Ruth and Bruce Rappaport Faculty of Medicine, Technion-Israel Institute of Technology, Haifa, Israel.
JNCI Cancer Spectr. 2019 May 2;3(2):pkz024. doi: 10.1093/jncics/pkz024. eCollection 2019 Jun.
A fecal test followed by diagnostic colonoscopy for a positive result is a widely endorsed screening strategy for colorectal cancer (CRC). However, the relationship between the time delay from the positive test to the follow-up colonoscopy and CRC mortality has not been established.
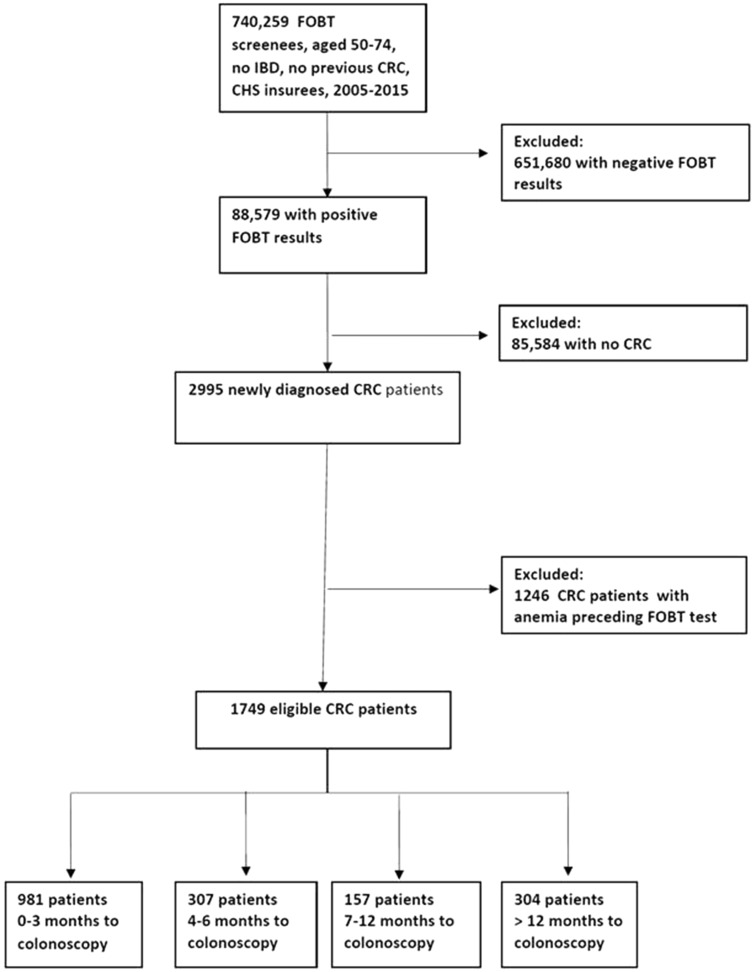
From a population-based screening program, we identified CRC patients newly diagnosed from 2005 through 2015 by a positive fecal occult test followed by a colonoscopy. The primary outcome measure was CRC-specific mortality according to four categories for the time elapsed between the positive result and the subsequent colonoscopy.
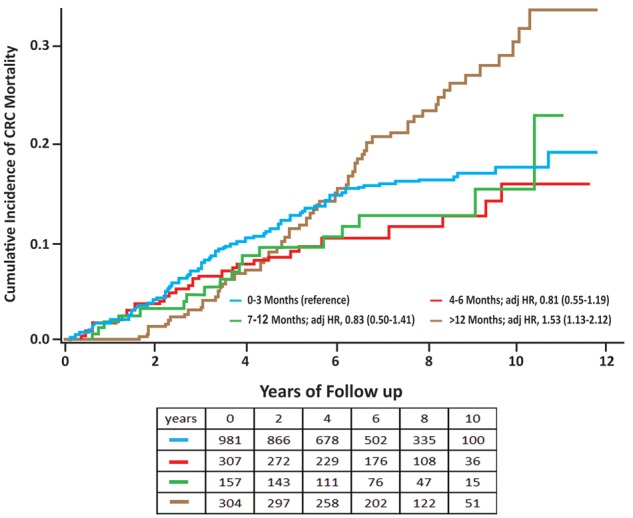
The 1749 patients underwent colonoscopies within 0-3 months (n = 981, 56.1%), 4-6 months (n = 307, 17.5%), 7-12 months (n = 157, 9.0%), and later than 12 months (n = 304, 17.4%). CRC-specific deaths according to exposure groups were: 13.8% (135 of 981) for 0-3 months, 10.7% (33 of 307) for 4-6 months (crude hazards ratio [HR] = 0.74, 95% confidence interval [CI] = 0.51 to 1.14), 11.5% (18 of 157) for 7-12 months (crude HR = 0.83, 95% CI = 0.51 to 1.42), and 22.7% (69 of 304) for longer than 12 months (crude HR = 1.40, 95% CI = 1.04 to 1.90). The only variable that was associated with mortality risk was the number of positive slides ( = .003). High positivity was twice the value in the 0-3 as the longer-than-12 months group: 51.9% vs 25.0% and similar for the 4-6 and 7-12 months groups (38.1% and 36.5%), respectively. The adjusted HRs for CRC mortality were 0.81 (95% CI = 0.55 to 1.19); 0.83 (95% CI = 0.50 to 1.41), and 1.53 (95% CI = 1.13 to 2.12, = .006) for the 4-12, 7-12, and longer-than-12-months groups, respectively, compared with the shortest delay group.
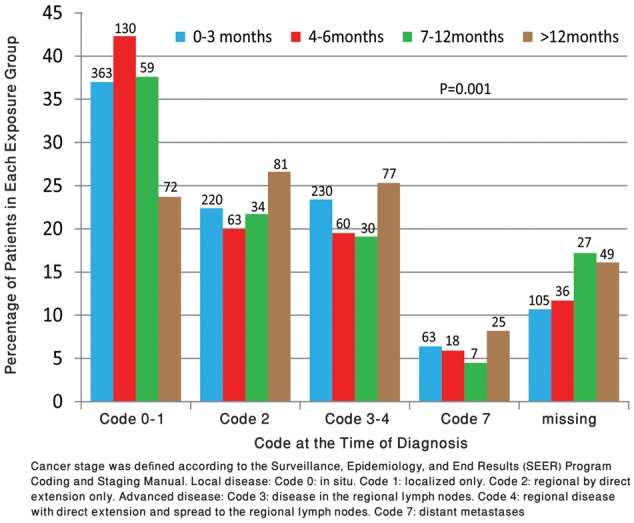
Among screen-diagnosed CRC patients, performance of colonoscopy more than 12 months after the initial positive fecal occult blood test was associated with more advanced disease and higher mortality due to CRC.
粪便检测后对阳性结果进行诊断性结肠镜检查是一种广泛认可的结直肠癌(CRC)筛查策略。然而,从阳性检测到后续结肠镜检查的时间延迟与CRC死亡率之间的关系尚未明确。
从一项基于人群的筛查项目中,我们识别出2005年至2015年间通过粪便潜血试验阳性后进行结肠镜检查而新诊断出的CRC患者。主要结局指标是根据阳性结果与后续结肠镜检查之间经过的时间分为四类的CRC特异性死亡率。
1749例患者在0 - 3个月内接受了结肠镜检查(n = 981,56.1%),4 - 6个月(n = 307,17.5%),7 - 12个月(n = 157,9.0%),以及12个月以后(n = 304,17.4%)。各暴露组的CRC特异性死亡情况如下:0 - 3个月组为13.8%(981例中的135例),4 - 6个月组为10.7%(307例中的33例)(粗危险比[HR] = 0.74,95%置信区间[CI] = 0.51至1.14),7 - 12个月组为11.5%(157例中的18例)(粗HR = 0.83,95% CI = 0.51至1.42),12个月以后组为22.7%(304例中的69例)(粗HR = 1.40,95% CI = 1.04至1.90)。与死亡风险相关的唯一变量是阳性玻片数量(P = 0.003)。高阳性率在0 - 3个月组是12个月以后组的两倍:分别为51.9%和25.0%,4 - 6个月组和7 - 12个月组相似(分别为38.1%和36.5%)。与最短延迟组相比,4 - 12个月、7 - 12个月和12个月以后组的CRC死亡率调整后HR分别为0.81(95% CI = 0.55至1.19);0.83(95% CI = 0.50至1.41),以及1.53(95% CI = 1.13至2.12,P = 0.006)。
在筛查诊断出的CRC患者中,初次粪便潜血试验阳性后12个月以上进行结肠镜检查与更晚期疾病及更高的CRC死亡率相关。