Paediatric Gastroenterology Hepatology and Nutrition, University Medical Center Groningen, University of Groningen, Groningen, the Netherlands.
J Pediatr Gastroenterol Nutr. 2019 Oct;69(4):466-473. doi: 10.1097/MPG.0000000000002458.
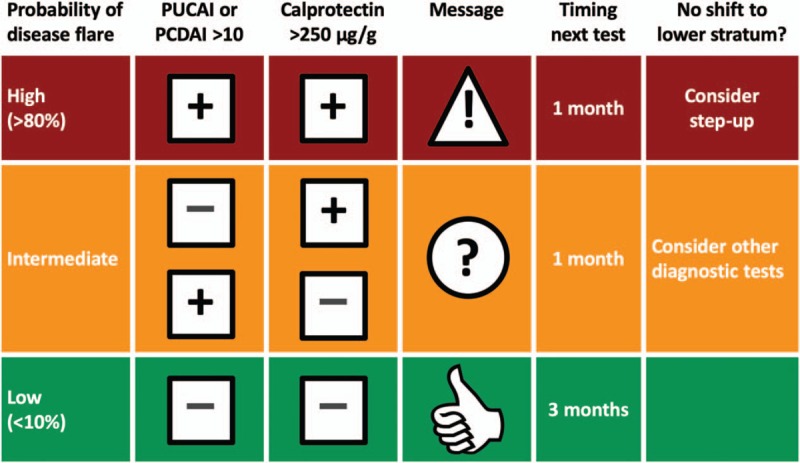
Treatment targets in inflammatory bowel disease (IBD) move away from controlling symptoms towards complete recovery of the intestinal mucosa. Currently, the most frequently used noninvasive surrogate marker of mucosal healing is a faecal calprotectin concentration in the target range. This study tested if there was a relation between time-to-reach target calprotectin and first flare.
We prospectively included new-onset IBD patients ages 17 and younger in a cloud-based registry (FastForwardCare) and followed them for at least 52 weeks. They were treated according to Dutch national guidelines that advocate a step-up approach. Time-to-reach target was defined as the first calprotectin measurement below 250 μg/g after the start of induction therapy. Time-to-first flare was the time from the first calprotectin measurement below 250 μg/g until reappearance of symptoms with calprotectin values above 250 μg/g.
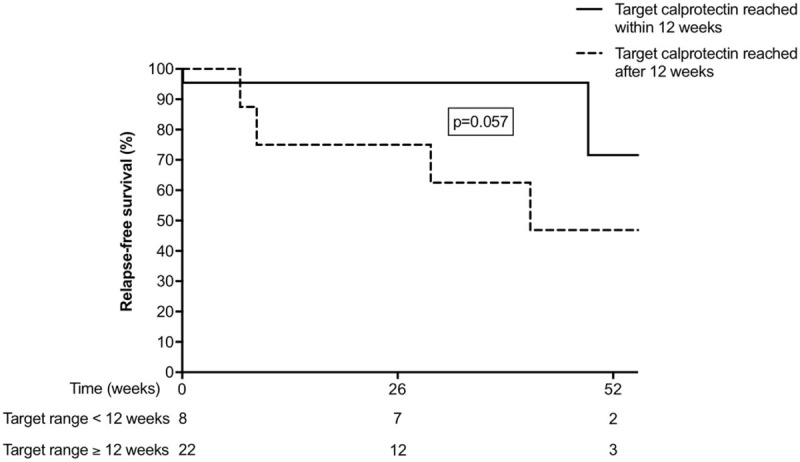
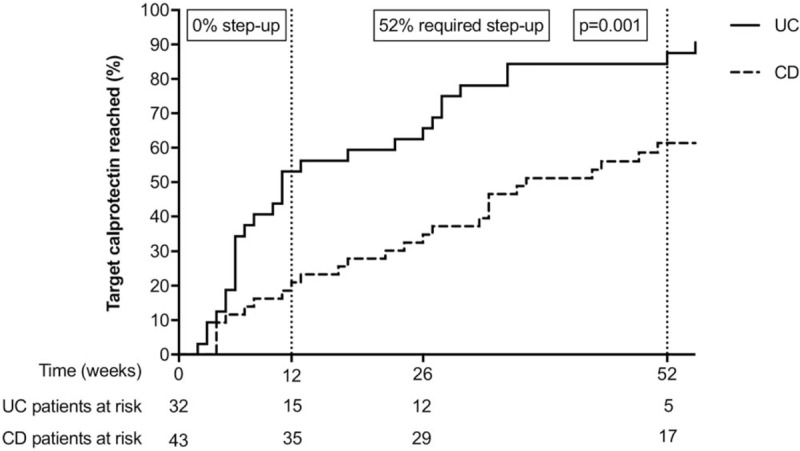
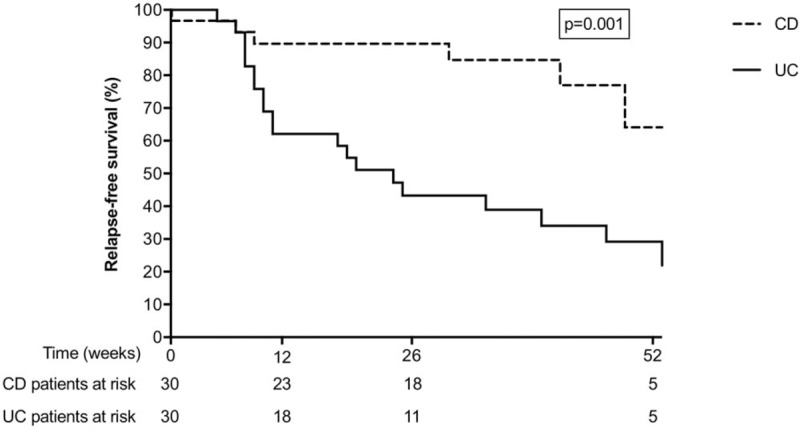
We included 76 patients (luminal Crohn disease [CD] 43); ulcerative colitis [UC] 33). Median age at diagnosis was, respectively 14.5 and 14.1 years. Median time-to-reach target calprotectin was 37 weeks in CD and 11 weeks in UC patients (Log-rank test, P = 0.001). Once the calprotectin target was reached, time-to-first flare was significantly longer in CD than in UC patients (Log-rank test, P = 0.001). CD patients with time-to-reach target calprotectin ≤12 weeks after conventional induction therapy (ie, exclusive enteral nutrition or steroids) had a more favorable disease course in the first year than those with time-to-reach target calprotectin >12 weeks (Log-rank test, P = 0.057). In UC patients, time-to-reach target calprotectin ≤12 weeks is not associated with a favorable disease course in the first year.
The findings of this prospective registry suggest that a quick response to conventional therapy predicts a favorable disease course in new-onset paediatric CD, but not in UC. The concept "time-to-reach target calprotectin level" rationalizes the indefinite term "response to treatment" and is well suited for studying treatment effectiveness in real-world practices.
炎症性肠病(IBD)的治疗目标已从控制症状转向完全恢复肠道黏膜。目前,最常用的黏膜愈合非侵入性替代标志物是靶目标范围内的粪便钙卫蛋白浓度。本研究测试了达到靶目标钙卫蛋白时间与首次复发之间是否存在关系。
我们前瞻性地在基于云的注册中心(FastForwardCare)中纳入了年龄在 17 岁及以下的新发 IBD 患者,并对他们进行了至少 52 周的随访。他们根据主张逐步治疗方法的荷兰国家指南进行治疗。达到目标时间定义为起始诱导治疗后首次钙卫蛋白测量值低于 250μg/g 后的第一次测量值。首次复发时间是指首次钙卫蛋白测量值低于 250μg/g 后至再次出现症状且钙卫蛋白值高于 250μg/g 的时间。
我们纳入了 76 例患者(肠克罗恩病[CD]43 例;溃疡性结肠炎[UC]33 例)。诊断时的中位年龄分别为 14.5 岁和 14.1 岁。CD 患者达到靶目标钙卫蛋白的中位时间为 37 周,UC 患者为 11 周(对数秩检验,P=0.001)。一旦达到钙卫蛋白目标值,CD 患者的首次复发时间明显长于 UC 患者(对数秩检验,P=0.001)。接受传统诱导治疗后达到靶目标钙卫蛋白时间≤12 周的 CD 患者(即,仅肠内营养或类固醇)在第一年的疾病过程中比达到靶目标钙卫蛋白时间>12 周的患者更有利(对数秩检验,P=0.057)。在 UC 患者中,达到靶目标钙卫蛋白时间≤12 周与第一年的有利疾病过程无关。
这项前瞻性登记研究的结果表明,对传统治疗的快速反应可预测新发性儿童 CD 的疾病过程有利,但对 UC 则不然。“达到靶目标钙卫蛋白水平的时间”这一概念使“治疗反应”这一不确定术语合理化,非常适合在实际实践中研究治疗效果。