Clinic for Anesthesiology and Critical Care Medicine, Rostock University Medical Center, Rostock, Germany.
Clinic for Anesthesiology, Intensive Care Medicine and Pain Therapy, University Hospital Muenster, Muenster, Germany.
PLoS One. 2019 Aug 1;14(8):e0220404. doi: 10.1371/journal.pone.0220404. eCollection 2019.
Patients experiencing cardiac arrest (CA) and cardiopulmonary resuscitation (CPR) often die or suffer from severe neurological impairment. Post resuscitation syndrome is characterized by a systemic inflammatory response. Toll-like receptor 4 (TLR4) is a major mediator of inflammation and TLR4 has been implicated in the pathogenesis of post-resuscitation encephalopathy. The aim of this study was to evaluate whether TLR4 deficiency or inhibition can modulate survival and neurofunctional outcome after CA/CPR.
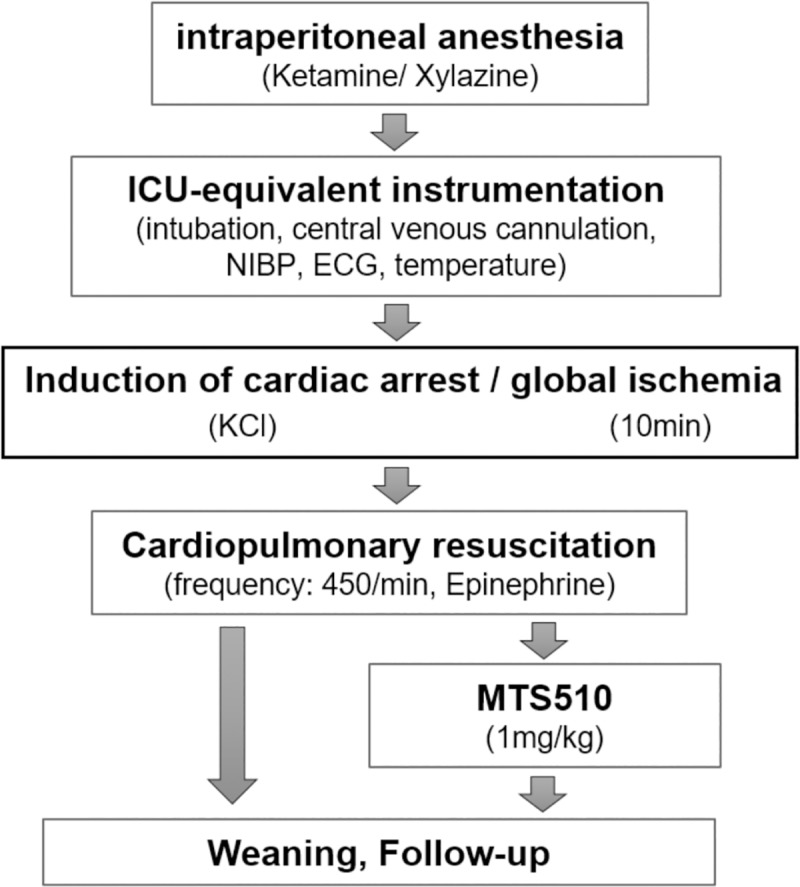
Following intubation and central venous cannulation, CA was induced in wild type (C57Bl/6J, n = 38), TLR4 deficient (TLR4-/-, n = 37) and TLR4 antibody treated mice (5mg/kg MTS510, n = 15) by high potassium. After 10min, CPR was performed using a modified sewing machine until return of spontaneous circulation (ROSC). Cytokines and cerebral TNFalpha levels were measured 8h after CA/CPR. Survival, early neurological recovery, locomotion, spatial learning and memory were assessed over a period of 28 days.
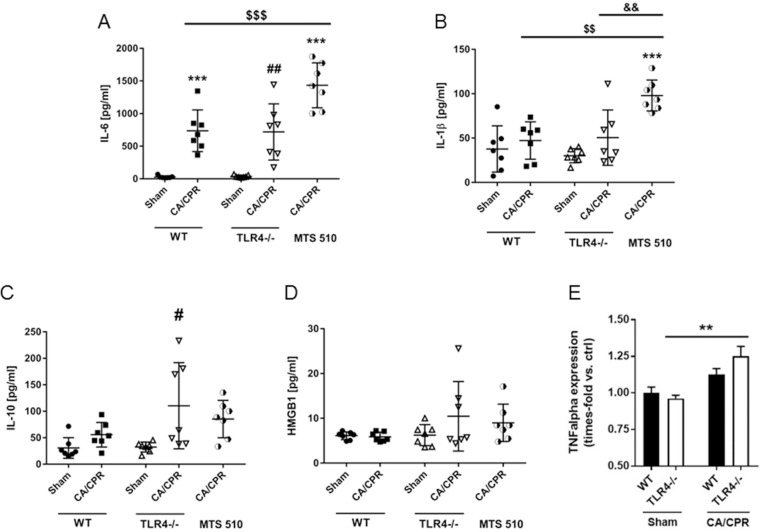
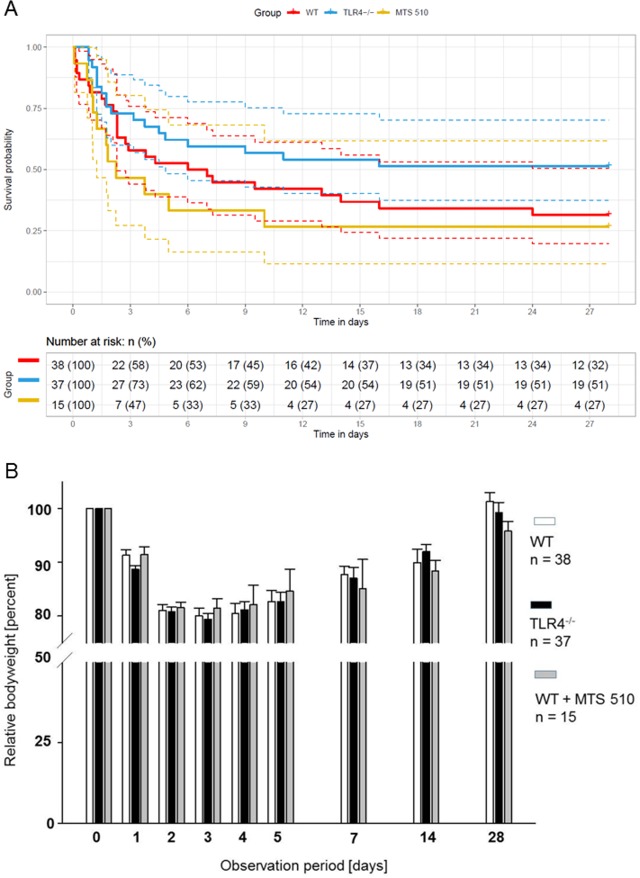
Following CA/CPR, all mice exhibited ROSC and 31.5% of wild type mice survived until day 28. Compared to wild type mice, neither TLR4-/- nor MTS510 treated wild type mice had statistically significant altered survival following CA/CPR (51.3 and 26.7%, P = 0.104 and P = 0.423 vs. WT, respectively). Antibody-treated but not TLR4-/- mice had higher IL-1β and IL-6 levels and TLR4-/- mice had higher IL-10 and cerebral TNFalpha levels. No differences existed between mice of all groups in early neurological recovery, locomotion, spatial learning ability or remembrance.
Therapeutic strategies targeting TLR4 may not be suitable for the reduction of mortality or neurofunctional impairment after CA/CPR.
经历心脏骤停 (CA) 和心肺复苏 (CPR) 的患者通常会死亡或遭受严重的神经功能障碍。复苏后综合征的特征是全身炎症反应。Toll 样受体 4 (TLR4) 是炎症的主要介质,TLR4 已被牵连到复苏后脑病的发病机制中。本研究旨在评估 TLR4 缺乏或抑制是否可以调节 CA/CPR 后的存活和神经功能结果。
在气管插管和中心静脉置管后,通过高钾诱导野生型 (C57Bl/6J,n = 38)、TLR4 缺陷型 (TLR4-/-,n = 37) 和 TLR4 抗体治疗的小鼠 (5mg/kg MTS510,n = 15) 发生 CA。10min 后,使用改良缝纫机进行 CPR,直到自主循环恢复 (ROSC)。CA/CPR 后 8h 测量细胞因子和大脑 TNFalpha 水平。在 28 天的时间内评估存活、早期神经恢复、运动、空间学习和记忆。
CA/CPR 后,所有小鼠均出现 ROSC,31.5%的野生型小鼠存活至第 28 天。与野生型小鼠相比,TLR4-/-或 MTS510 治疗的野生型小鼠在 CA/CPR 后存活率没有统计学上的显著改变 (51.3%和 26.7%,P = 0.104 和 P = 0.423 与 WT 相比,分别)。抗体治疗但不是 TLR4-/-小鼠的 IL-1β 和 IL-6 水平更高,而 TLR4-/-小鼠的 IL-10 和大脑 TNFalpha 水平更高。所有组之间的小鼠在早期神经恢复、运动、空间学习能力或记忆方面没有差异。
针对 TLR4 的治疗策略可能不适合降低 CA/CPR 后的死亡率或神经功能障碍。