Department of Radiation Oncology, Klinikum rechts der Isar, Technical University Munich, Ismaninger Str. 22, D-81675, Munich, Germany.
Department of Radiation Oncology, University Hospital Zurich, University of Zurich, Rämistrasse 100, CH-8091, Zurich, Switzerland.
Radiat Oncol. 2019 Aug 1;14(1):135. doi: 10.1186/s13014-019-1328-7.
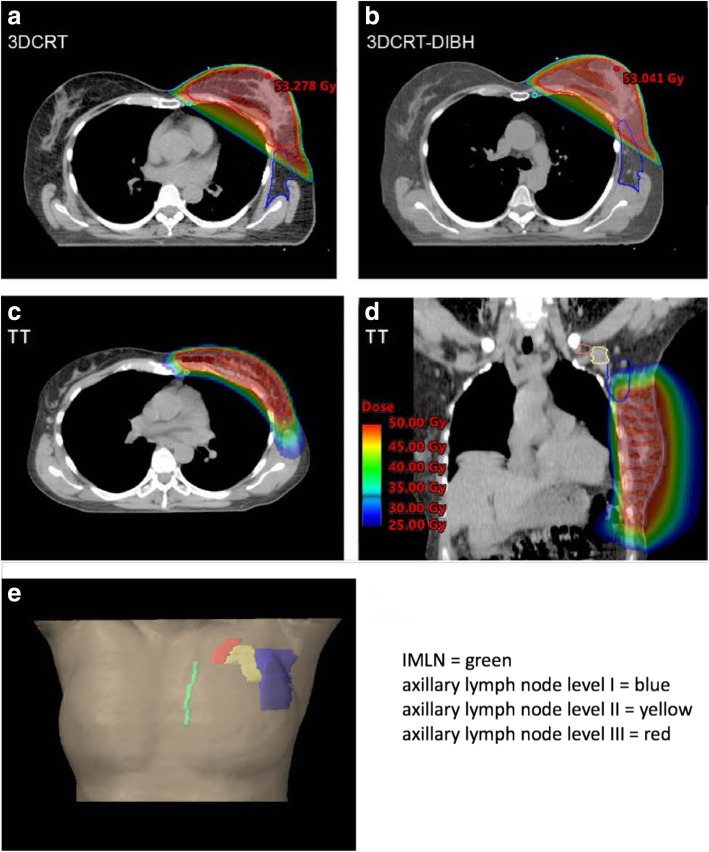
PURPOSE/OBJECTIVE(S): Along with breast-conserving surgery (BCS), adjuvant radiotherapy (RT) of patients with early breast cancer plays a crucial role in the oncologic treatment concept. Conventionally, irradiation is carried out with the aid of tangentially arranged fields. However, more modern and more complex radiation techniques such as IMRT (intensity-modulated radio therapy) are used more frequently, as they improve dose conformity and homogeneity and, in some cases, achieve better protection of adjacent risk factors. The use of this technique has implications for the incidental- and thus unintended- irradiation of adjacent loco regional lymph drainage in axillary lymph node levels I-III and internal mammary lymph nodes (IMLNs). A comparison of a homogeneous "real-life" patient collective, treated with helical tomotherapy (TT), patients treated with 3D conformal RT conventional tangentially arranged fields (3DCRT) and deep inspiration breath hold (3DCRT-DIBH), was conducted.
MATERIALS/METHODS: This study included 90 treatment plans after BCS, irradiated in our clinic from January 2012 to August 2016 with TT (n = 30) and 3D-CRT (n = 30), 3DCRT DIBH (n = 30). PTVs were contoured at different time points by different radiation oncologists (> 7). TT was performed with a total dose of 50.4 Gy and a single dose of 1.8 Gy with a simultaneous integrated boost (SIB) to the tumor cavity (TT group). Patients irradiated with 3DCRT/3DCRT DIBH received 50 Gy à 2 Gy and a sequential boost. Contouring of lymph drainage routes was performed retrospectively according to RTOG guidelines.
Average doses (DMean) in axillary lymph node Level I/Level II/Level III were 31.6 Gy/8.43 Gy/2.38 Gy for TT, 24.0 Gy/11.2 Gy/3.97 Gy for 3DCRT and 24.7 Gy/13.3 Gy/5.59 Gy for 3DCRT-DIBH patients. Internal mammary lymph nodes (IMLNs) Dmean were 27.8 Gy (TT), 13.5 Gy (3DCRT), and 18.7 Gy (3DCRT-DIBH). Comparing TT to 3DCRT-DIBH dose varied significantly in all axillary lymph node levels and the IMLNs. Comparing TT to 3DCRT significant dose difference in Level I and IMLNs was observed.
Dose applied to locoregional lymph drainage pathways varies comparing tomotherapy plans to conventional tangentially arranged fields. Studies are warranted whether dose variations influence loco-regional spread and must have implications for target volume definition guidelines.
保乳手术后(BCS),辅助放疗(RT)在早期乳腺癌的治疗中起着至关重要的作用。传统上,通过切线野进行照射。然而,更现代和更复杂的放射技术,如调强放射治疗(IMRT),使用得越来越频繁,因为它们可以提高剂量的一致性和均匀性,在某些情况下,还可以更好地保护相邻的危险因素。该技术的使用会导致腋窝淋巴结水平 I-III 和内乳淋巴结(IMLN)的相邻局部区域淋巴结引流的意外(即非故意)照射。对一组接受螺旋断层放疗(TT)、三维适形放疗常规切线野(3DCRT)和深吸气屏气(3DCRT-DIBH)治疗的同质“真实患者”群体进行了比较。
材料/方法:本研究包括 2012 年 1 月至 2016 年 8 月在我院接受 BCS 治疗后 90 例治疗计划,其中 TT(n=30)和 3D-CRT(n=30)、3DCRT-DIBH(n=30)。不同时间点由不同的放射肿瘤学家(>7)对 PTV 进行了轮廓勾画。TT 采用总剂量 50.4Gy,单次剂量 1.8Gy,同时对肿瘤腔进行同步整合增敏(SIB)(TT 组)。接受 3DCRT/3DCRT-DIBH 照射的患者接受 50Gy 2Gy,序贯加量。根据 RTOG 指南回顾性勾画淋巴结引流途径。
TT 患者腋淋巴结 I 级/II 级/III 级的平均剂量(Dmean)分别为 31.6Gy/8.43Gy/2.38Gy,3DCRT 患者分别为 24.0Gy/11.2Gy/3.97Gy,3DCRT-DIBH 患者分别为 24.7Gy/13.3Gy/5.59Gy。内乳淋巴结(IMLN)的 Dmean 分别为 27.8Gy(TT)、13.5Gy(3DCRT)和 18.7Gy(3DCRT-DIBH)。与 3DCRT-DIBH 相比,TT 患者在所有腋窝淋巴结水平和 IMLNs 中的剂量差异显著。与 3DCRT 相比,TT 患者 I 级和 IMLNs 的剂量差异有统计学意义。
与传统切线野相比,调强放疗计划应用于局部区域淋巴结引流途径的剂量不同。需要研究剂量变化是否会影响局部区域扩散,并对靶区定义指南产生影响。