Icon Cancer Centre, Level 4, The Epworth Centre, 32 Erin Street, Richmond, Victoria, 3121, Australia.
Icon Cancer Centre, Mulgrave, Victoria, 3170, Australia.
Radiat Oncol. 2019 Dec 10;14(1):223. doi: 10.1186/s13014-019-1430-x.
The addition of regional nodal radiation (RNI) to whole breast irradiation for high risk breast cancer improves metastases free survival and new data suggests it contributes additional benefit to overall survival. Deep inspiration breath hold (DIBH) has been shown to reduce cardiac and pulmonary dose in the context of left-sided disease treated with or without RNI, yet few studies have investigated its utility for right-breast cancer. This study investigates the potential advantages of DIBH in local and locoregional radiotherapy for right-sided breast cancer.
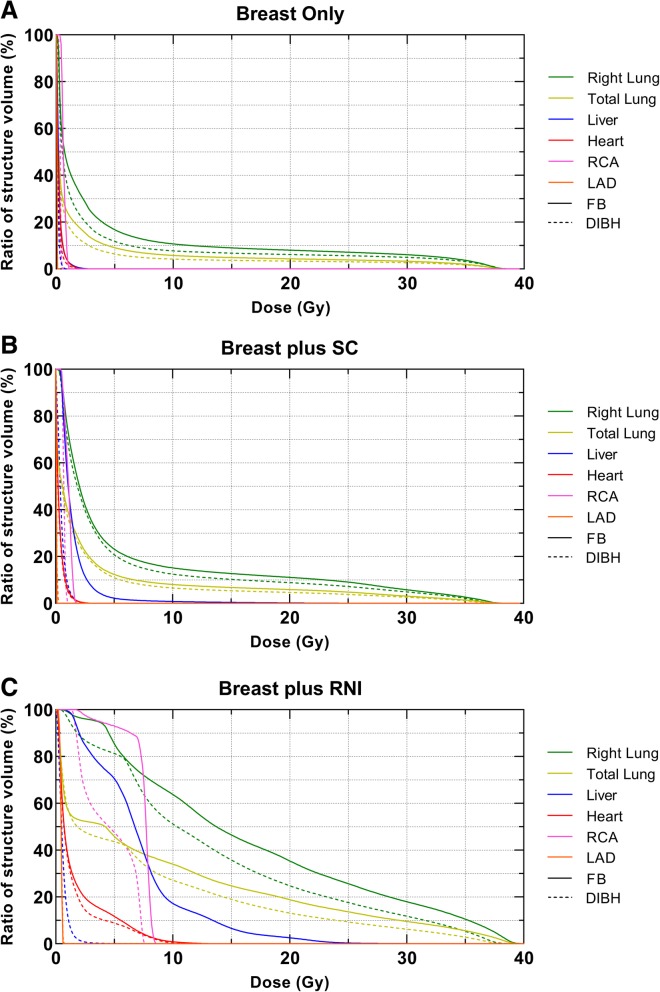
Free-breathing (FB) and DIBH computed tomography datasets were obtained from twenty patients who previously underwent radiotherapy for left-sided breast cancer. Ten patients were retrospectively planned for whole right breast only irradiation and ten patients were planned for irradiation to the whole breast plus ipsilateral supra-clavicular (SC) nodes, with and without irradiation of the ipsilateral internal mammary nodes (IMN). Dose-volume metrics for the clinical target volume, lungs, heart, left anterior descending artery, right coronary artery (RCA) and liver were recorded. Differences between FB and DIBH plans were analysed using Wilcoxon signed-rank tests, with P < 0.05 considered statistically significant.
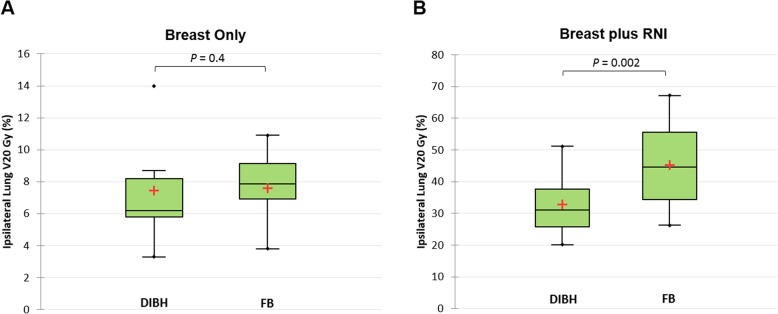
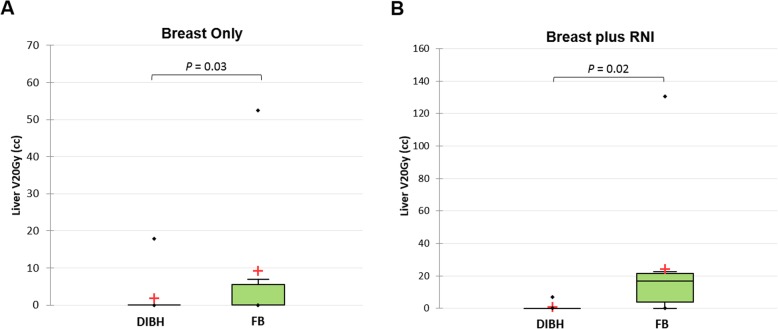
DIBH increased the average total lung volume compared to FB in both breast only and breast plus RNI cohorts (P = 0.001). For the breast only group, there was no significant improvement in any ipsilateral lung dose-volume metric between FB and DIBH. However, for the breast plus RNI group, there was an improvement in ipsilateral lung mean dose (18.9 ± 3.2 Gy to 15.9 ± 2.3 Gy, P = 0.002) and V20Gy (45.3 ± 13.3% to 32.9 ± 9.4%, P = 0.002). In addition, DIBH significantly reduced the maximum dose to the RCA for RNI (11.6 ± 7.2 Gy to 5.6 ± 2.9 Gy, P = 0.03). Significant reductions in the liver V20Gy and maximum dose were observed in all cohorts during DIBH compared to FB.
DIBH is a promising approach for right-breast radiotherapy with considerable sparing of normal tissue, particularly when the ipsilateral IMNs are also irradiated.
对于高危乳腺癌患者,在全乳照射的基础上增加区域淋巴结照射(RNI)可改善无转移生存,新数据表明其对总生存也有额外获益。深吸气屏气(DIBH)已被证明可降低左侧疾病接受或不接受 RNI 治疗时的心脏和肺剂量,但很少有研究探讨其在右侧乳腺癌中的应用。本研究探讨了 DIBH 在右侧乳腺癌局部和局部区域放疗中的潜在优势。
从 20 例先前接受左侧乳腺癌放疗的患者中获得自由呼吸(FB)和 DIBH 计算机断层扫描数据集。对 10 例患者进行回顾性全右乳照射计划,10 例患者进行全乳加同侧锁骨上(SC)淋巴结照射计划,其中 5 例加同侧内乳淋巴结(IMN)照射。记录临床靶体积、肺、心脏、左前降支、右冠状动脉(RCA)和肝脏的剂量-体积参数。使用 Wilcoxon 符号秩检验分析 FB 和 DIBH 计划之间的差异,P 值<0.05 被认为具有统计学意义。
与 FB 相比,DIBH 在仅行乳房照射和乳房加 RNI 两组中均增加了平均全肺体积(P=0.001)。在仅行乳房照射组中,FB 和 DIBH 之间同侧肺任何剂量-体积参数均无显著改善。然而,在乳房加 RNI 组中,同侧肺平均剂量(18.9±3.2 Gy 至 15.9±2.3 Gy,P=0.002)和 V20Gy(45.3±13.3%至 32.9±9.4%,P=0.002)有所改善。此外,DIBH 显著降低了加行 RNI 时 RCA 的最大剂量(11.6±7.2 Gy 至 5.6±2.9 Gy,P=0.03)。与 FB 相比,所有组在 DIBH 时均显著降低了肝脏 V20Gy 和最大剂量。
DIBH 是一种很有前途的右侧乳腺癌放疗方法,可显著减少正常组织的照射,特别是当同侧 IMN 也被照射时。