Westhoff D, Engelen-Lee J Y, Hoogland I C M, Aronica E M A, van Westerloo D J, van de Beek D, van Gool W A
1Department of Neurology, Amsterdam Neuroscience, Amsterdam University Medical Center, University of Amsterdam, Amsterdam, Netherlands.
3Department of Neuropathology, Amsterdam University Medical Center, University of Amsterdam, Amsterdam, Netherlands.
Immun Ageing. 2019 Jul 30;16:18. doi: 10.1186/s12979-019-0158-7. eCollection 2019.
Systemic infection is associated with long-term cognitive deficits and functional decline. In this study we hypothesized that severe systemic inflammation leads to a neuroinflammatory response that is characterized by microglial activation, and that these effects might be more pronounced in patients using medication with anticholinergic side-effects.
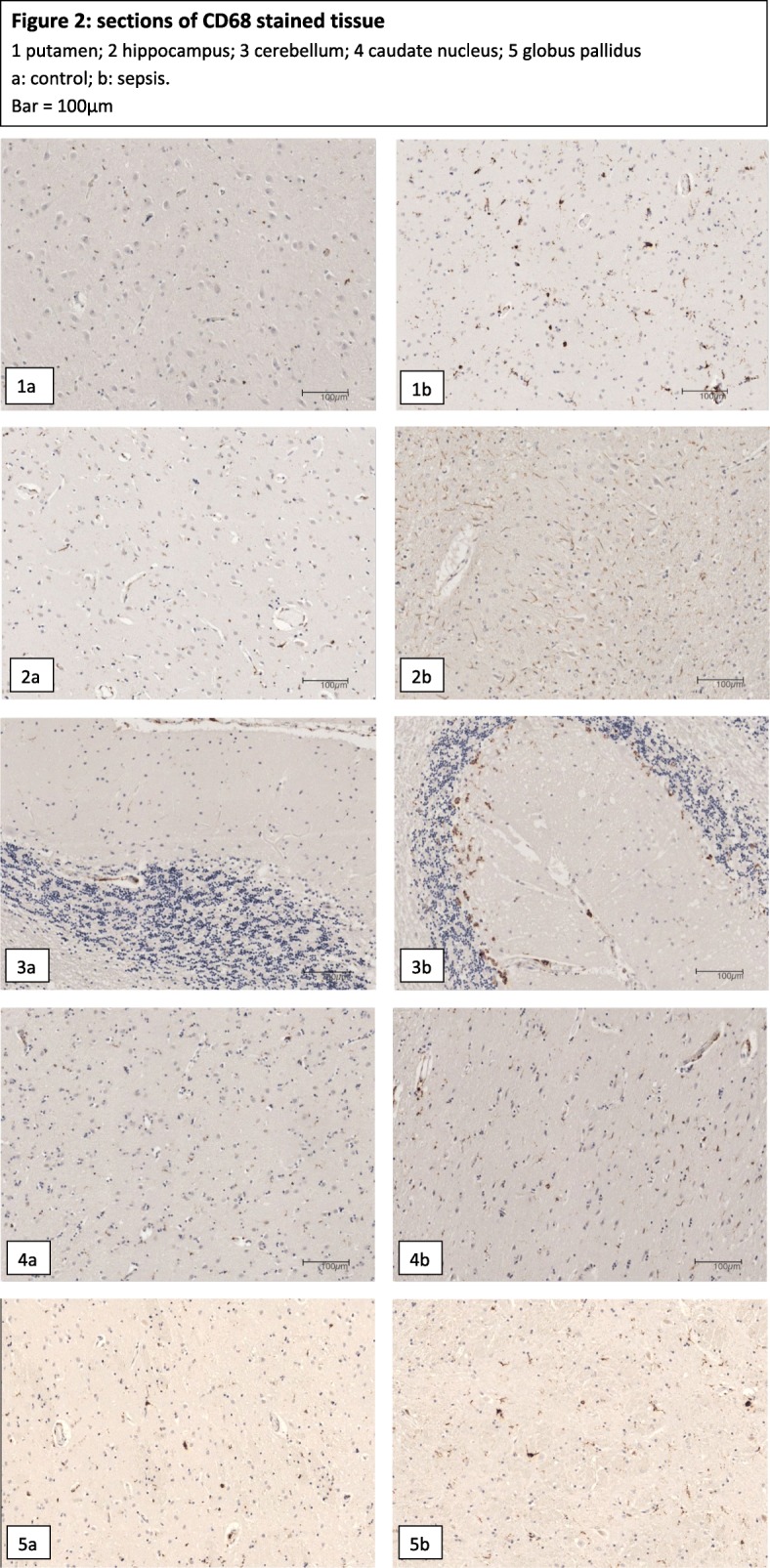
Based on the results of a pilot study in 8 patients, we assessed the number of MHC-II and CD-68 positive cells by immunohistochemistry and compared the number of microglia in specific brain regions of 16 well-characterized patients with septic shock and 15 controls.
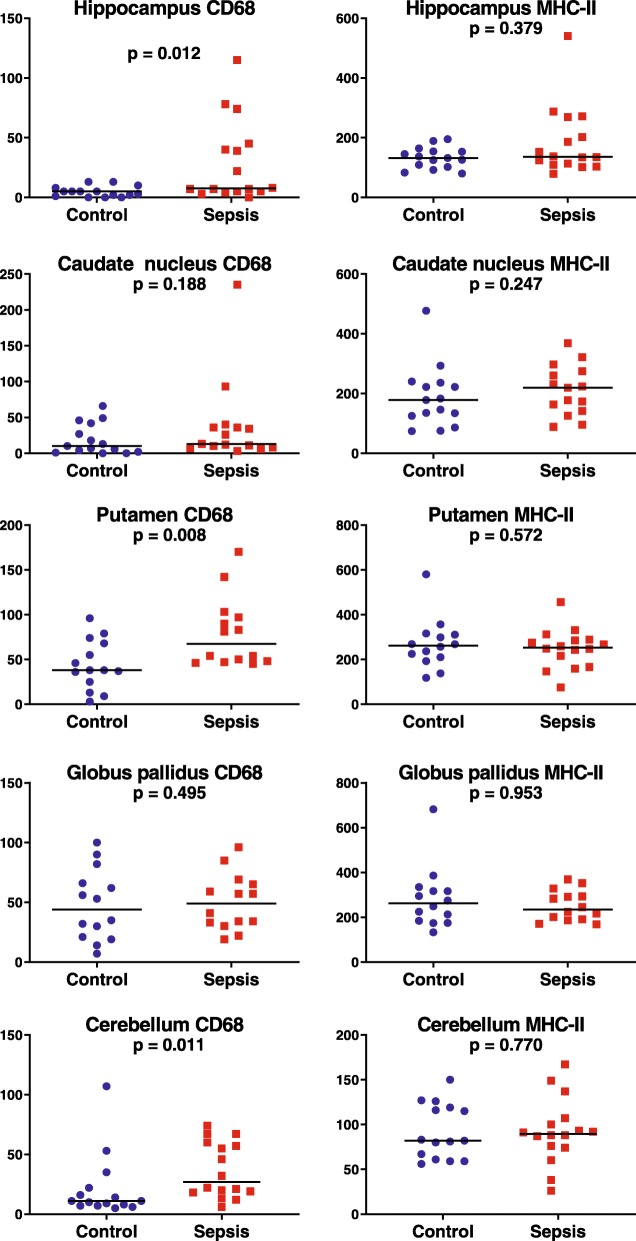
In the pilot study, patients with sepsis tended to have higher density of MHC-II and CD-68 positive microglia in the basal ganglia (putamen, caudate nucleus and globus pallidus) and of MHC-II positive microglia in the hippocampus. In the validation study, patients with sepsis had a significantly higher number of CD-68 positive cells in hippocampus (1.5 fold; = 0.012), putamen (2.2 fold; = 0.008) and cerebellum (2.5 fold; = 0.011) than control patients. The density of MHC-II positive microglia was similar between sepsis and control groups. There was no consistent correlation between microglia counts and anti-cholinergic activity drugs score.
In patients who die during septic shock, severe systemic inflammation is accompanied by localized and strong upregulation of CD-68 positive microglia, but not of MHC-II positive microglia. We identified regional differences in the brain with increased microglial activation in putamen, hippocampus and cerebellum.
全身感染与长期认知缺陷和功能衰退有关。在本研究中,我们假设严重的全身炎症会导致以小胶质细胞激活为特征的神经炎症反应,并且这些影响在使用具有抗胆碱能副作用药物的患者中可能更为明显。
基于对8例患者的初步研究结果,我们通过免疫组织化学评估了MHC-II和CD-68阳性细胞的数量,并比较了16例明确诊断为感染性休克患者和15例对照者特定脑区的小胶质细胞数量。
在初步研究中,脓毒症患者基底节(壳核、尾状核和苍白球)中MHC-II和CD-68阳性小胶质细胞的密度以及海马中MHC-II阳性小胶质细胞的密度往往较高。在验证研究中,脓毒症患者海马(1.5倍;P = 0. .012)、壳核(2.2倍;P = 0.008)和小脑(2.5倍;P = 0.011)中CD-68阳性细胞的数量明显高于对照患者。脓毒症组和对照组之间MHC-II阳性小胶质细胞的密度相似。小胶质细胞计数与抗胆碱能活性药物评分之间没有一致的相关性。
在感染性休克期间死亡的患者中,严重的全身炎症伴随着CD-68阳性小胶质细胞的局部和强烈上调,但MHC-II阳性小胶质细胞没有。我们发现壳核、海马和小脑中脑区小胶质细胞激活增加存在差异。