Department of Clinical and Molecular Medicine, Faculty of Medicine, NTNU, Norwegian University of Science and Technology, Trondheim, Norway.
The Cancer Clinic, St. Olav's Hospital, Trondheim University Hospital, Trondheim, Norway.
J Cachexia Sarcopenia Muscle. 2019 Dec;10(6):1347-1355. doi: 10.1002/jcsm.12469. Epub 2019 Aug 6.
Studies show that low skeletal muscle index (SMI) and low skeletal muscle density (SMD) are negative prognostic factors and associated with more toxicity from systemic therapy in cancer patients. However, muscle depletion can be caused by a range of diseases, and many cancer patients have significant co-morbidity. The aim of this study was to investigate whether there were associations between co-morbidity and muscle measures in patients with advanced non-small cell lung cancer.
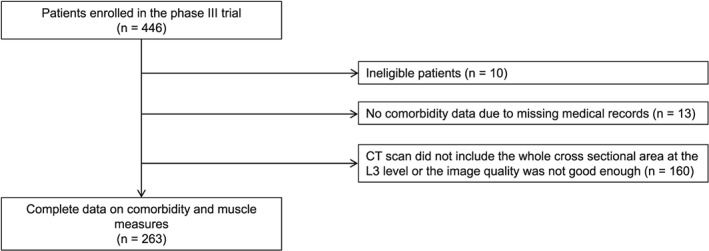
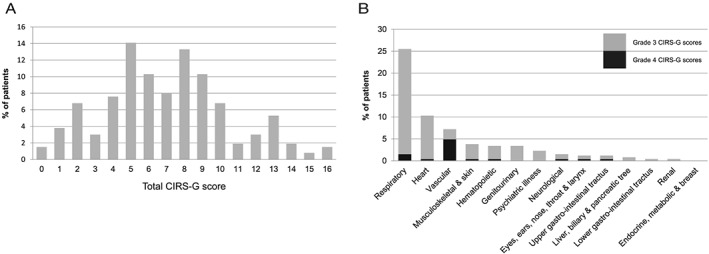
Patients in a Phase III trial comparing two chemotherapy regimens in advanced non-small cell lung cancer were analysed (n = 436). Co-morbidity was assessed using the Cumulative Illness Rating Scale for Geriatrics (CIRS-G), which rates co-morbidity from 0 to 4 on 14 different organ scales. Severe co-morbidity was defined as having any grades 3 and 4 CIRS-G score. Muscle measures were assessed from baseline computed tomography slides at the L3 level using the SliceOMatic software.
Complete data were available for 263 patients (60%). Median age was 66, 57.0% were men, 78.7% had performance status 0-1, 25.9% Stage IIIB, 11.4% appetite loss, 92.4% were current/former smokers, 22.8% were underweight, 43.7% had normal weight, 26.6% were overweight, and 6.8% obese. The median total CIRS-G score was 7 (range: 0-16), and 48.2% had severe co-morbidity. Mean SMI was 44.7 cm /m (range: 27-71), and the mean SMD was 37.3 Hounsfield units (HU) (range: 16-60). When comparing patients with and without severe co-morbidity, there were no significant differences in median SMI (44.5 vs. 44.1 cm /m ; 0.70), but patients with severe co-morbidity had a significantly lower median SMD (36 HU vs. 39 HU; 0.001), mainly due to a significant difference in SMD between those with severe heart disease and those without (32.5 vs. 37.9 HU; 0.002). Linear regression analyses confirmed the association between severe co-morbidity and SMD both in the simple analysis (0.001) and the multiple analysis (0.037) adjusting for baseline characteristics. Stage of disease, gender, and body mass index (BMI) were significantly associated with SMI in both the simple and multiple analyses. Age and BMI were significantly associated with SMD in the simple analysis; and age, gender, and BMI were significantly associated in the multiple analysis.
There were no significant differences in SMI between patients with and patients without severe co-morbidity, but patients with severe co-morbidity had lower SMD than other patients, mainly due to severe heart disease. Co-morbidity might be a confounder in studies of the clinical role of SMD in cancer patients.
研究表明,低骨骼肌指数(SMI)和低骨骼肌密度(SMD)是癌症患者的负面预后因素,并与全身治疗的更多毒性相关。然而,肌肉消耗可能由一系列疾病引起,许多癌症患者有明显的合并症。本研究旨在探讨晚期非小细胞肺癌患者的合并症与肌肉指标之间是否存在关联。
对比较两种化疗方案在晚期非小细胞肺癌中的疗效的 III 期试验中的患者进行分析(n=436)。使用累积疾病评分量表(CIRS-G)评估合并症,该量表根据 14 个不同器官的评分将合并症分为 0 到 4 级。严重合并症定义为任何等级 3 和 4 的 CIRS-G 评分。从基线计算机断层扫描片(L3 水平)使用 SliceOMatic 软件评估肌肉指标。
263 名患者(60%)的完整数据可用。中位年龄为 66 岁,57.0%为男性,78.7%的体能状态为 0-1 级,25.9%为 IIIB 期,11.4%为食欲丧失,92.4%为当前/曾经吸烟者,22.8%为体重不足,43.7%为体重正常,26.6%为超重,6.8%为肥胖。总 CIRS-G 评分中位数为 7(范围:0-16),48.2%有严重合并症。平均 SMI 为 44.7cm/m(范围:27-71),平均 SMD 为 37.3 亨氏单位(HU)(范围:16-60)。比较有严重合并症和无严重合并症的患者,SMI 的中位数无显著差异(44.5 与 44.1cm/m;0.70),但有严重合并症的患者 SMD 中位数明显较低(36 HU 与 39 HU;0.001),主要是由于严重心脏病患者与无严重心脏病患者之间的 SMD 存在显著差异(32.5 与 37.9 HU;0.002)。线性回归分析在简单分析(0.001)和调整基线特征的多元分析(0.037)中均证实了严重合并症与 SMD 之间的关联。在简单和多元分析中,疾病分期、性别和体重指数(BMI)均与 SMI 显著相关。年龄和 BMI 与 SMD 显著相关,在简单分析中;年龄、性别和 BMI 在多元分析中显著相关。
有严重合并症和无严重合并症的患者之间的 SMI 无显著差异,但有严重合并症的患者的 SMD 较低,主要是由于严重心脏病。合并症可能是癌症患者 SMD 临床作用研究中的一个混杂因素。