Liver Unit Queen Elizabeth Hospital Birmingham UK.
Institute of Translational Medicine University Hospitals Birmingham NHS Foundation Trust Birmingham UK.
BJS Open. 2019 Apr 2;3(4):476-484. doi: 10.1002/bjs5.50161. eCollection 2019 Aug.
Early treatment is the only potential cure for periampullary cancer. The pathway to surgery is complex and involves multiple procedures across local and specialist hospitals. The aim of this study was to analyse variability within this pathway, and its impact on cost and outcomes.
Patients undergoing surgery for periampullary cancer (2011-2016) were identified retrospectively and their pathway to surgery was analysed. Patients who had early surgery (shortest quartile, Q1) were compared with those having late surgery (longest quartile, Q4).
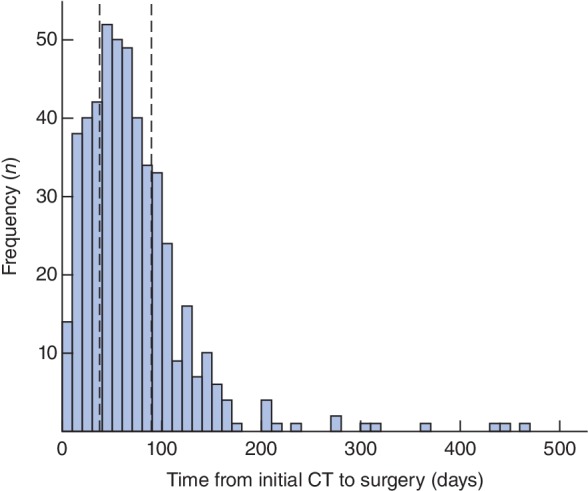
A total of 483 patients were included in the study, with 121 and 124 patients in Q1 and Q4 respectively. The median time from initial CT to surgery was 21 days for Q1 112 days for Q4 ( < 0·001). Diagnostic delays were common in Q4; these patients required significantly more investigations than those in Q1 (endoscopic ultrasonography (EUS): 74·2 18·2 per cent respectively, < 0·001; MRI: 33·6 20·6 per cent, = 0·036). The median time to diagnostic EUS was 13 days in Q1 59 days in Q4 ( < 0·001). Some 42·1 per cent of jaundiced patients in Q1 underwent preoperative biliary drainage, compared with all patients in Q4. There were significantly more unplanned admissions and associated longer duration of hospital stay per patient and costs in Q4 than in Q1 (median: 8 3 days respectively; €5652 €2088; both < 0·001). There was a higher likelihood of potentially curative surgery in Q1 (82·6 per cent 66·9 per cent in Q4; = 0·005).
There is wide variation across the entire pathway, suggesting that multiple strategies are required to enable early surgery. Defining an effective pathway by anticipating the need for investigations and avoiding biliary drainage reduces unplanned admissions and costs and increases resection rates.
早期治疗是治疗壶腹周围癌的唯一潜在方法。到达手术的路径复杂,涉及当地和专科医院的多个程序。本研究的目的是分析该途径中的变异性及其对成本和结果的影响。
回顾性地确定了 2011 年至 2016 年间接受壶腹周围癌手术的患者,并分析了他们到达手术的途径。将接受早期手术(最短四分位数,Q1)的患者与接受晚期手术(最长四分位数,Q4)的患者进行比较。
共有 483 名患者纳入研究,Q1 和 Q4 组分别有 121 名和 124 名患者。从初始 CT 到手术的中位时间为 Q1 为 21 天,Q4 为 112 天( < 0·001)。Q4 中诊断延迟很常见;与 Q1 相比,这些患者需要进行更多的检查(内镜超声检查(EUS):分别为 74.2 18.2%, < 0·001;磁共振成像(MRI):33.6 20.6%, = 0·036)。Q1 中诊断性 EUS 的中位时间为 13 天,Q4 中为 59 天( < 0·001)。在 Q1 中,42.1%的黄疸患者接受了术前胆道引流,而 Q4 中所有患者均接受了该治疗。Q4 中计划外住院和相关住院时间以及每位患者的费用均明显高于 Q1(中位数:8 3 天;€5652 €2088;均 < 0·001)。在 Q1 中,更有可能进行潜在的治愈性手术(82.6% 66.9%在 Q4; = 0·005)。
整个途径存在广泛的差异,表明需要采取多种策略才能实现早期手术。通过预测检查需求和避免胆道引流来确定有效的途径,可以减少计划外住院和成本,并提高切除率。