Molecular Pathology Research Center, Department of Pathology, Peking Union Medical College Hospital, Peking Union Medical College, Chinese Academy of Medical Sciences, Beijing, China.
Department of Breast Surgery, Peking Union Medical College Hospital, Peking Union Medical College, Chinese Academy of Medical Sciences, Beijing, China.
Breast Cancer Res Treat. 2019 Nov;178(2):275-281. doi: 10.1007/s10549-019-05387-6. Epub 2019 Aug 6.
Human epidermal growth factor receptor 2 (HER2) status is both an independent prognostic factor and a predictive factor for the efficacy of targeted therapy for breast cancer, so it is critical to accurately detect HER2 protein expression and/or gene amplification. According to the recommendations of the 2013 American Society of Clinical Oncology and College of American Pathologists (ASCO/CAP) guidelines for HER2 breast cancer testing, an additional test should be pursued on a different block from the same tumor as one of the options for patients with immunohistochemistry (IHC) 2+ and a HER2/CEP17 ratio of < 2.0 with an average HER2 signals per tumor cell of ≥ 4.0 and < 6.0 by reflex test using dual-probe fluorescence in situ hybridization (FISH) (double-equivocal HER2). Our aim in this study is to explore the consistency of HER2 status between the two blocks.
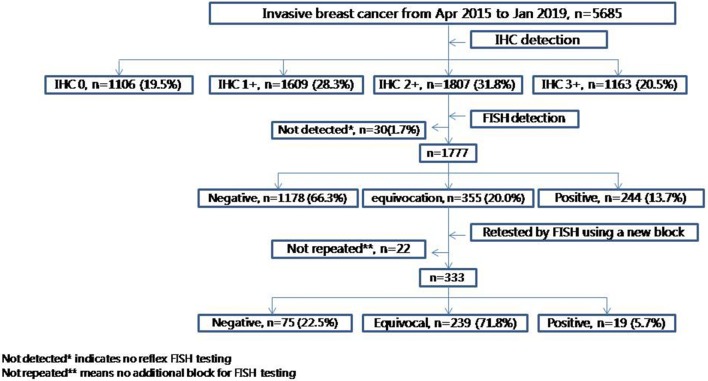
We retrospectively analyzed 5685 primary invasive breast cancers between April 2015 and January 2019 from Peking Union Medical College Hospital. For cases with double-equivocal HER2 revealed in initial blocks, HER2 gene status was evaluated by FISH in a different block from the same tumor. The FISH score was interpreted according to the 2013 ASCO/CAP guidelines for HER2 testing.
In our cohort of 5685 specimens, the overall HER2 IHC3+, 2+, 1+ and 0 cases were 20.5%, 31.8%, 28.3%, and 19.5%, respectively. Then, 13.7%, 66.3%, and 20.0% of HER2 amplification, non-amplification, and equivocation rates were found, respectively, in IHC2+ patients (n = 1777) by reflex FISH assay. For specimens with double-equivocal HER2 (n = 333), HER2 status was assessed in another block from the same tumor by FISH and then the frequency of HER2 positive, negative, and equivocation was estimated at 5.7%, 22.5%, and 71.8%, respectively. Because double-equivocal HER2 cases are classified in the HER2 negative category by the 2018 ASCO/CAP HER2 testing guidelines, only 1.3% (19/1511) of HER2 positive patients were determined through additional HER2 testing in another block from the HER2 negative population.
HER2 status in different blocks from the same tumor in primary invasive breast cancer was highly concordant. Our data supported the recommendation of the 2018 ASCO/CAP HER2 testing guidelines in breast cancer to remove the suggestion for additional HER2 testing using another block contained in the previous version.
人表皮生长因子受体 2(HER2)状态既是乳腺癌的独立预后因素,也是靶向治疗疗效的预测因素,因此准确检测 HER2 蛋白表达和/或基因扩增至关重要。根据 2013 年美国临床肿瘤学会和美国病理学家协会(ASCO/CAP)HER2 乳腺癌检测指南的建议,对于免疫组织化学(IHC)2+且 HER2/CEP17 比值<2.0 的患者,一种选择是对同一肿瘤的另一个肿瘤块进行额外检测,该肿瘤块的平均每个肿瘤细胞的 HER2 信号≥4.0 且<6.0,使用双探针荧光原位杂交(FISH)进行反射性检测(双临界 HER2)。我们在这项研究中的目的是探讨同一肿瘤的两个肿瘤块之间 HER2 状态的一致性。
我们回顾性分析了 2015 年 4 月至 2019 年 1 月期间北京协和医学院医院的 5685 例原发性浸润性乳腺癌病例。对于初始肿瘤块中出现双临界 HER2 的病例,使用来自同一肿瘤的另一个肿瘤块通过 FISH 评估 HER2 基因状态。根据 2013 年 ASCO/CAP HER2 检测指南解读 FISH 评分。
在我们的 5685 例标本队列中,HER2 IHC3+、2+、1+和 0 的总体病例分别为 20.5%、31.8%、28.3%和 19.5%。然后,在 IHC2+患者(n=1777)中通过反射 FISH 检测发现 HER2 扩增、非扩增和不确定率分别为 13.7%、66.3%和 20.0%。对于双临界 HER2(n=333)的标本,通过 FISH 检测评估了另一个来自同一肿瘤的肿瘤块,然后估计了 HER2 阳性、阴性和不确定的频率分别为 5.7%、22.5%和 71.8%。由于 2018 年 ASCO/CAP HER2 检测指南将双临界 HER2 病例归类为 HER2 阴性,因此仅在 HER2 阴性人群中,通过来自 HER2 阴性肿瘤的另一个肿瘤块的额外 HER2 检测确定了 1.3%(19/1511)的 HER2 阳性患者。
同一肿瘤的不同肿瘤块中的 HER2 状态高度一致。我们的数据支持 2018 年 ASCO/CAP HER2 检测指南在乳腺癌中的建议,即删除之前版本中包含的使用另一个肿瘤块进行额外 HER2 检测的建议。