Neglected Tropical Disease Programme, Ghana Health Services (GHS), Accra, Ghana.
Department of Parasitology, Noguchi Memorial Institute for Medical Research (NMIMR), College of Health Sciences, University of Ghana, Legon, Ghana.
PLoS Negl Trop Dis. 2019 Aug 9;13(8):e0007115. doi: 10.1371/journal.pntd.0007115. eCollection 2019 Aug.
Ghana started its national programme to eliminate lymphatic filariasis (LF) in 2000, with mass drug administration (MDA) with ivermectin and albendazole as main strategy. We review the progress towards elimination that was made by 2016 for all endemic districts of Ghana and analyze microfilaria (mf) prevalence from sentinel and spot-check sites in endemic districts.
We reviewed district level data on the history of MDA and outcomes of transmission assessment surveys (TAS). We further collated and analyzed mf prevalence data from sentinel and spot-check sites.
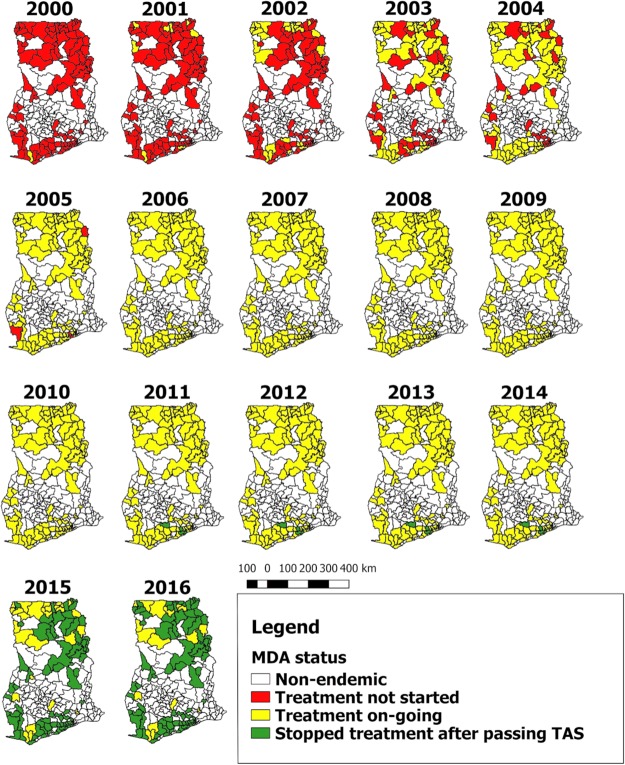
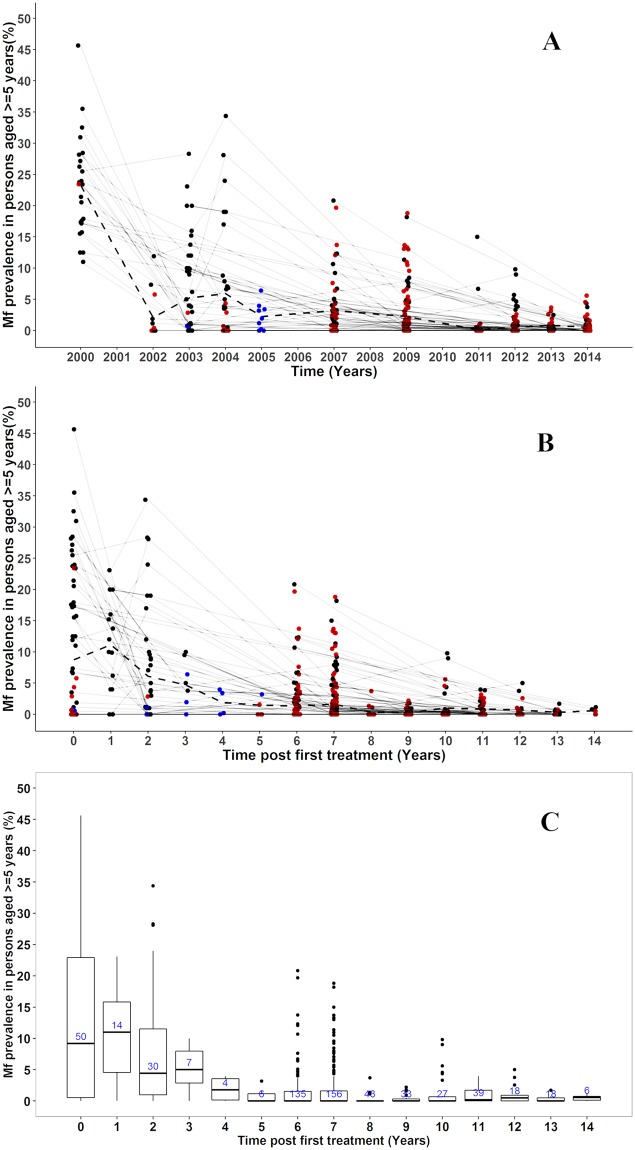
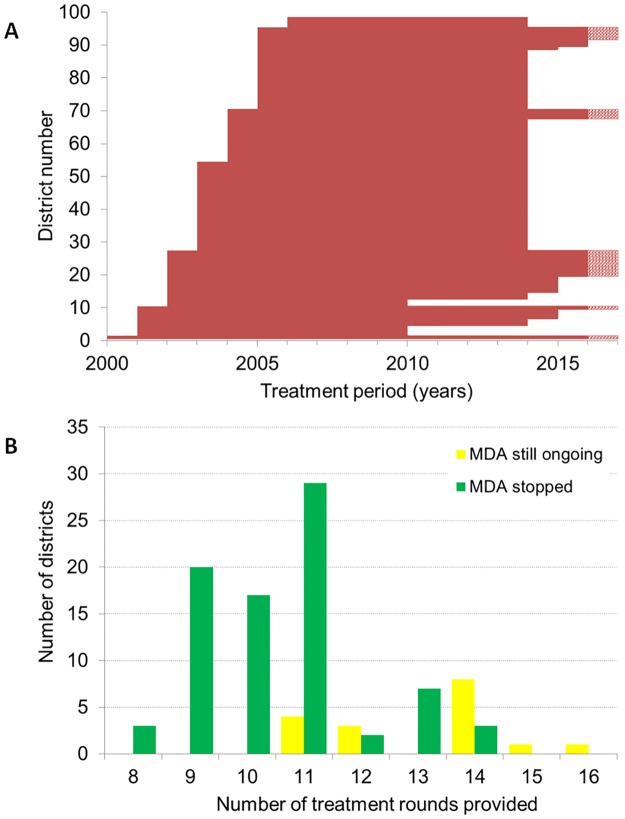
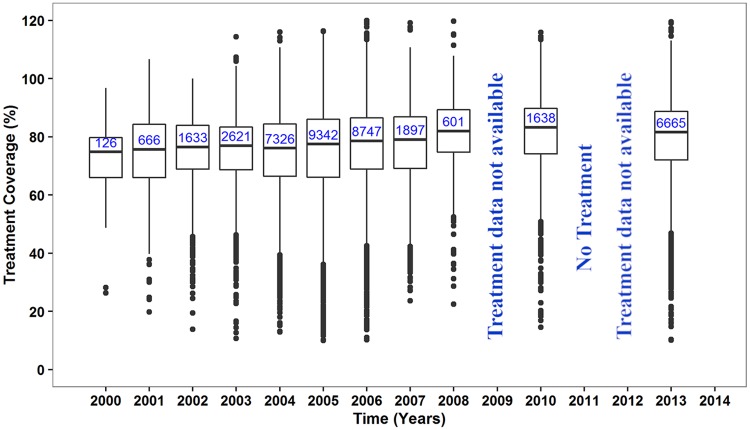
MDA was initiated in 2001-2006 in all 98 endemic districts; by the end of 2016, 81 had stopped MDA after passing TAS and after an average of 11 rounds of treatment (range 8-14 rounds). The median reported coverage for the communities was 77-80%. Mf prevalence survey data were available for 430 communities from 78/98 endemic districts. Baseline mf prevalence data were available for 53 communities, with an average mf prevalence of 8.7% (0-45.7%). Repeated measurements were available for 78 communities, showing a steep decrease in mean mf prevalence in the first few years of MDA, followed by a gradual further decline. In the 2013 and 2014 surveys, 7 and 10 communities respectively were identified with mf prevalence still above 1% (maximum 5.6%). Fifteen of the communities above threshold are all within districts where MDA was still ongoing by 2016.
The MDA programme of the Ghana Health Services has reduced mf prevalence in sentinel sites below the 1% threshold in 81/98 endemic districts in Ghana, yet 15 communities within 13 districts (MDA ongoing by 2016) had higher prevalence than this threshold during the surveys in 2013 and 2014. These districts may need to intensify interventions to achieve the WHO 2020 target.
加纳于 2000 年启动国家淋巴丝虫病(LF)消除规划,以伊维菌素和阿苯达唑为主要策略的大规模药物治疗(MDA)。我们回顾了 2016 年加纳所有流行地区消除工作的进展情况,并分析了流行地区哨点和抽查点的微丝蚴(mf)流行率。
我们回顾了 MDA 历史和传播评估调查(TAS)结果的地区数据。我们进一步整理和分析了来自哨点和抽查点的 mf 流行率数据。
2001-2006 年,所有 98 个流行地区均启动 MDA;截至 2016 年底,81 个地区在通过 TAS 并完成 11 轮(8-14 轮)治疗后停止 MDA。报告的社区覆盖率中位数为 77-80%。78/98 个流行地区的 430 个社区有 mf 流行率调查数据。53 个社区有基线 mf 流行率数据,平均 mf 流行率为 8.7%(0-45.7%)。78 个社区有重复测量数据,表明 MDA 实施的头几年 mf 流行率急剧下降,随后逐渐进一步下降。在 2013 年和 2014 年的调查中,分别有 7 个和 10 个社区 mf 流行率仍高于 1%(最高为 5.6%)。在 2016 年仍在进行 MDA 的 13 个地区中,有 15 个社区的 mf 流行率超过阈值。
加纳卫生服务部的 MDA 规划使加纳 98 个流行地区中的 81 个地区的哨点 mf 流行率降至 1%以下,但在 2013 年和 2014 年的调查中,13 个地区的 15 个社区的流行率高于该阈值。这些地区可能需要加强干预措施,以实现世卫组织 2020 年的目标。