1School of Medicine and Health Management, Tongji Medical School, Huazhong University of Science and Technology, Wuhan, Hubei China.
2School of Psychology and Public Health, La Trobe University, Melbourne, Victoria Australia.
Antimicrob Resist Infect Control. 2019 Aug 7;8:132. doi: 10.1186/s13756-019-0592-5. eCollection 2019.
Irrational use of antibiotics is a major driver of development of antibiotic resistance, which heavily threatens population health worldwide. Understanding the mechanism of physician's antibiotic prescribing decisions is increasingly highlighted to promote prudent use of antibiotics. Therefore, the current study aimed to fill the gap, modelling physician's antibiotic prescribing and identifying the potential intrinsic and external determinants of antibiotic prescribing in primary care.
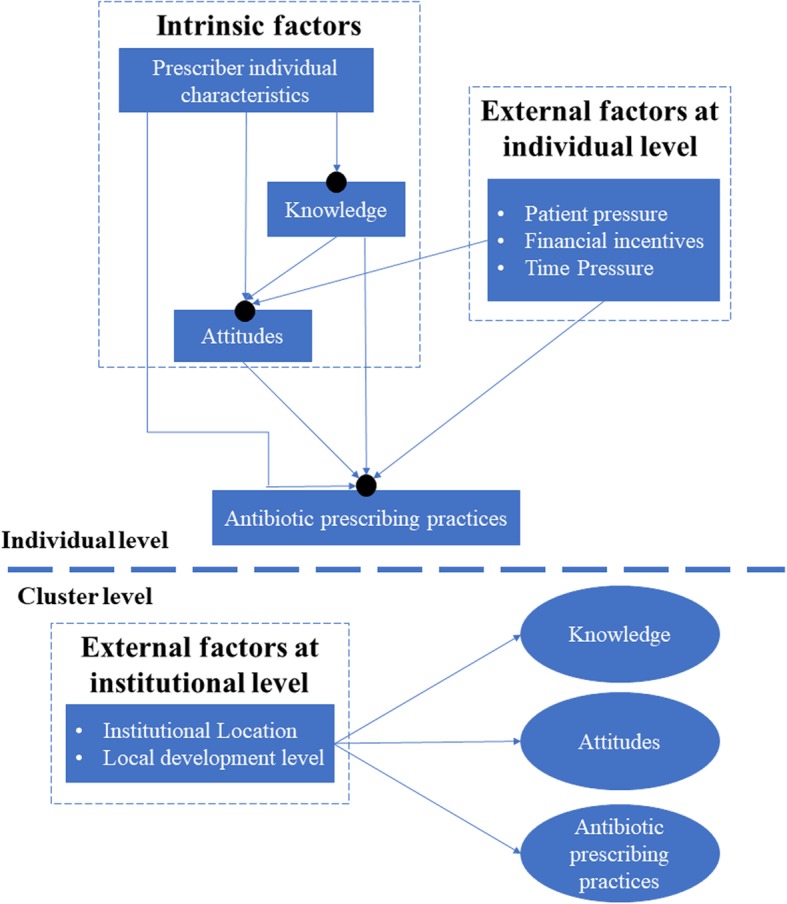
A total of 428,475 prescriptions from 499 prescribers in 65 primary care facilities in Hubei of China were audited. Teixeira Antibiotic Prescribing Behavioral Model (TAPBM) was referred as theoretical basis to identify intrinsic and external predictors of antibiotic prescriptions. A questionnaire survey was conducted, covering potential physician's intrinsic determinants (knowledge, attitudes and individual characteristics) and external factors both in individual level (patient pressure, time pressure and financial incentives) and institutional level (setting and local socio-economic development). A two-level path analysis was performed linking potential determinants of antibiotic use with physician's actual practices.
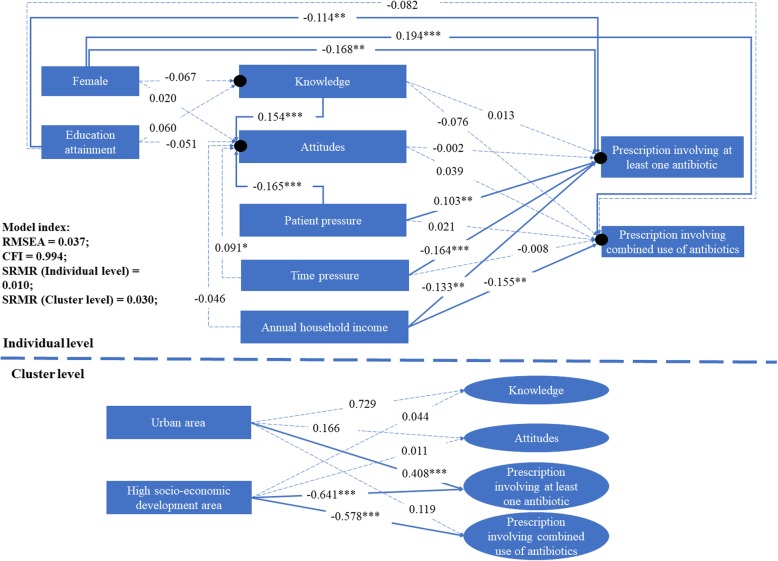
About 44.28% of the prescriptions contained antibiotics, with 9.28% containing two or more antibiotics. The multi-level path analysis revealed that knowledge was a significant predictor of attitudes (β = 0.154, < 0.05), but higher knowledge and attitudes failed to translate into antibiotic prescribing practices ((β = - 0.076 - 0.039, > 0.05). Instead, external factors played a more important role and physician's antibiotic use was significantly associated with patient pressure (β = 0.102, = 0.022), time pressure (β = - 0.164, = 0.002), financial incentives (β = - 0.133- - 0.155, = 0.027) and institutional environments (rural area, β = 0.408, = 0.002; and high socioeconomic setting, β = - 0.641 - -0.578, < 0.001 ). The prescribers who were male (β = - 0.168, = 0.007) or had lower qualification (β = - 0.114, = 0.028) were also more likely to prescribe antibiotics than others.
Antibiotic prescribing practices are complex process and associated with both intrinsic (prescriber) and external (patients and institutional environment) factors. A systematic approach is required to curb over-prescription of antibiotics. Apart from educating prescribers, it is equally important, if not more, to educate patients, break incentives and nurture professional culture within organization to reduce the overuse of antibiotics.
抗生素的不合理使用是抗生素耐药性发展的主要驱动因素,这对全球人口健康造成了严重威胁。了解医生开抗生素处方的机制对于促进抗生素的合理使用越来越受到重视。因此,本研究旨在填补空白,对初级保健中的医生抗生素处方进行建模,并确定抗生素处方的潜在内在和外在决定因素。
对来自中国湖北省 65 个基层医疗机构的 499 名医生开具的 428475 张处方进行审核。Teixeira 抗生素处方行为模型(TAPBM)被作为理论依据,以确定抗生素处方的内在和外在预测因素。进行了一项问卷调查,涵盖了潜在医生的内在决定因素(知识、态度和个体特征)以及个体层面(患者压力、时间压力和经济激励)和机构层面(环境和当地社会经济发展)的外在因素。进行了两级路径分析,将抗生素使用的潜在决定因素与医生的实际实践联系起来。
约 44.28%的处方含有抗生素,其中 9.28%的处方含有两种或两种以上抗生素。多水平路径分析显示,知识是态度的一个显著预测因素(β=0.154, < 0.05),但较高的知识和态度并没有转化为抗生素的使用(β=-0.076-0.039, > 0.05)。相反,外部因素发挥了更重要的作用,医生的抗生素使用与患者压力(β=0.102, = 0.022)、时间压力(β=-0.164, = 0.002)、经济激励(β=-0.133- -0.155, = 0.027)和机构环境(农村地区,β=0.408, = 0.002;高社会经济环境,β=-0.641 - -0.578, < 0.001)显著相关。男性医生(β=-0.168, = 0.007)或资质较低的医生(β=-0.114, = 0.028)开具抗生素处方的可能性也高于其他医生。
抗生素处方行为是一个复杂的过程,与内在(医生)和外在(患者和机构环境)因素有关。需要采取系统的方法来遏制抗生素的过度使用。除了教育医生外,教育患者、打破激励机制和培养组织内的专业文化同样重要,以减少抗生素的过度使用。