1School of Medicine and Health Management, Tongji Medical School, Huazhong University of Science and Technology, Wuhan, Hubei China.
2School of Psychology and Public Health, La Trobe University, Melbourne, Vic Australia.
Antimicrob Resist Infect Control. 2019 Jan 30;8:23. doi: 10.1186/s13756-019-0478-6. eCollection 2019.
Over-prescription of antibiotics is prevalent all over the world, contributing to the development of antibiotic resistance. The importance of understanding how physicians prescribe antibiotics is increasingly highlighted for the purpose of promoting good practice. This study aimed to identify factors that shape the antibiotic prescribing behaviors of physicians in primary care based on the theory of planned behavior (TPB).
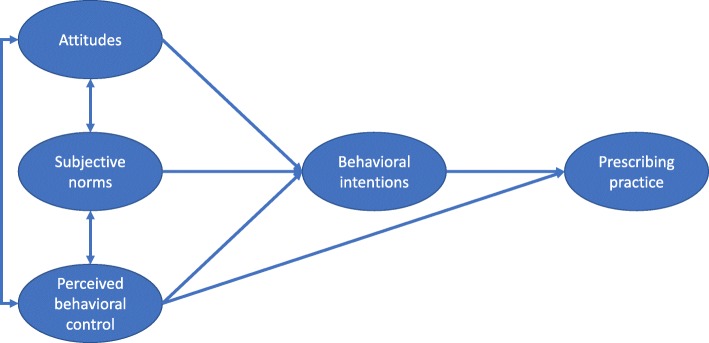
Data were collected from 503 prescribers within 65 primary care facilities in Hubei, tapping into four behavioral aspects leading to antibiotic prescribing based on TPB, namely, attitudes (the degree to which a prescriber is in favor of the use of antibiotics), subjective norms (perceived social pressure to which a prescriber is subject in relation to antibiotic prescriptions), perceived control of behaviors (how easy a prescriber feels in making a rational decision on antibiotic prescriptions) and intentions (the degree to which a prescriber is willing to prescribe antibiotics). A total of 440,268 prescriptions were audited to assess physician antibiotic prescribing practices. The four behavioral constructs were further linked with physician's actual use of antibiotics using structural equation modelling (SEM) based on TPB.
On average, 40.54% (SD = 20.82%) of the outpatient encounters resulted in a prescription for an antibiotic given by the participants and 9.81% (SD = 10.18%) of the patients were given two or more antibiotics. The participants showing a more favorable attitude toward antibiotics had a higher intention to prescribe antibiotics (β = 0.226, < 0.001) and a lower intention to reduce antibiotic use (β = - 0.211, < 0.001). Those who perceived lower social pressure (β = 0.113, = 0.030) and higher control over prescribing behaviors (β = 0.113, = 0.037) reported a higher intention to reduce the use of antibiotics. However, such intention did not translate into prescribing practice ( > 0.05), although stronger perceived behavioral control was directly linked with lower antibiotic prescriptions (β = - 0.110, = 0.019). Weaker perceived behavioral control was evident in the participants who showed a less favorable attitude toward antibiotics (β = 0.128, = 0.001).
Antibiotic prescribing practice is not under the volitional control of prescribers in primary care in China. Their rational prescribing practice is likely to be jeopardized by perceived weak control over prescribing behaviors.
抗生素的过度处方在全球范围内普遍存在,导致抗生素耐药性的产生。了解医生开抗生素的方式对于促进良好实践至关重要。本研究旨在根据计划行为理论(TPB),确定影响初级保健医生开抗生素行为的因素。
本研究在湖北的 65 家基层医疗机构中,对 503 名开处方者进行了数据收集,根据 TPB,共涉及四个导致抗生素处方的行为方面,分别为态度(医生开抗生素的程度)、主观规范(医生在抗生素处方方面受到的社会压力)、行为控制感(医生在开抗生素处方方面的决策的难易程度)和意向(医生开抗生素的意愿程度)。共审核了 440268 张处方,以评估医生的抗生素处方行为。使用基于 TPB 的结构方程模型(SEM)将这四个行为结构与医生的实际抗生素使用情况进一步联系起来。
平均而言,40.54%(SD=20.82%)的门诊就诊患者获得了参与者开出的抗生素处方,9.81%(SD=10.18%)的患者开了两种或两种以上的抗生素。对抗生素持更有利态度的参与者有更高的开抗生素意向(β=0.226, < 0.001)和更低的减少抗生素使用意向(β=-0.211, < 0.001)。那些认为社会压力较小(β=0.113, = 0.030)和对处方行为控制感较高(β=0.113, = 0.037)的人报告称,减少抗生素使用的意向更高。然而,这种意向并没有转化为开处方的行为( > 0.05),尽管更强的感知行为控制与较低的抗生素处方直接相关(β=-0.110, = 0.019)。在对抗生素态度不那么有利的参与者中,感知行为控制较弱(β=0.128, = 0.001)。
中国初级保健医生的抗生素处方行为不受医生的意志控制。他们的合理处方行为可能因感知到的处方行为控制能力较弱而受到威胁。