Tripathy Jaya Prasad, Sagili Karuna D, Kathirvel Soundappan, Trivedi Archana, Nagaraja Sharath Burugina, Bera Om Prakash, Reddy Kiran Kumar, Satyanarayana Srinath, Khanna Ashwani, Chadha Sarabjit S
Centre for Operational Research, International Union Against Tuberculosis and Lung Disease, New Delhi, India.
Centre for Operational Research, International Union Against Tuberculosis and Lung Disease, Paris, France.
Diabetes Metab Syndr Obes. 2019 Jul 19;12:1189-1199. doi: 10.2147/DMSO.S192336. eCollection 2019.
Weak public health systems have been identified as major bottlenecks in providing good quality diabetic care in low- and middle-income countries.
The present study assessed diabetic care services at public health facilities across six districts in three states of India using a mixed methods approach. The study described diabetes care services available at public health facilities and identified challenges and solutions needed to tackle them. The quantitative component included assessment of availability of services and resources, whilst the qualitative component was comprised of semistructured interviews with health care providers and persons with diabetes to understand the pathway of care.
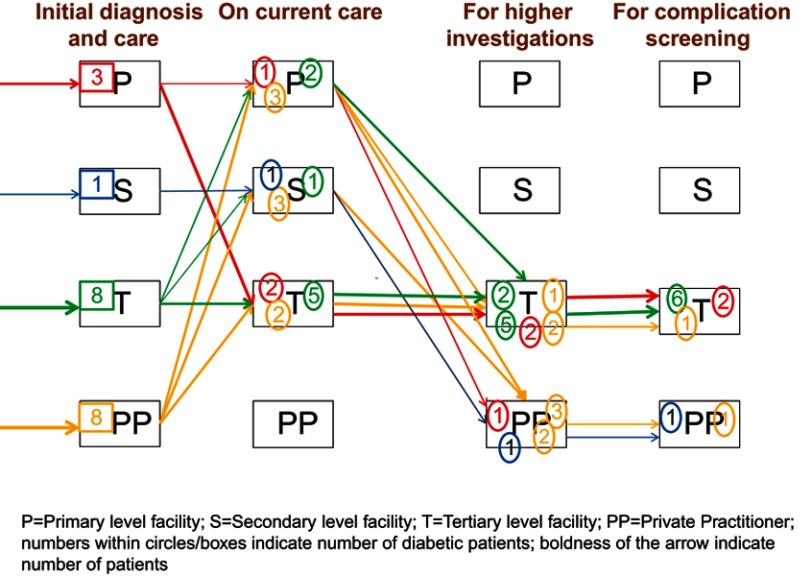
A total of 30 health facilities were visited: five tertiary; eight secondary and 17 primary health facilities. Patient clinical records were not maintained at the facilities; the onus was on patients to keep their own clinical records. All had the facility for blood glucose measurement, but HbA1c estimation was available only at tertiary centers. None of the primary health centers in the three states provided HbA1c estimation, lipid examination, or foot care. Lifestyle modification support was available in only a few tertiary facilities. Antidiabetic drugs (biguanides and sulphonyl ureas) were available in most facilities, and given for 14 days. Insulin and statins were available only at secondary and tertiary care centers. Forty-two physicians were interviewed and poor follow-up, patient overload, and lack of specialized training were the major barriers that emerged from the interview responses. A total of 37 patients were interviewed. Patients had to visit tertiary facilities for drugs and routine follow-up, thereby congesting the facilities. There was no formal referral or follow-up mechanism to link patients to decentralized facilities.
There is a wide gap between effective diabetes management practices and their implementation. There should be a greater role of secondary care facilities in follow-up investigations and screening for complications. A holistic diabetic care package with a robust recording and cohort monitoring system and adequate referral mechanism is needed.
在低收入和中等收入国家,薄弱的公共卫生系统已被视为提供高质量糖尿病护理的主要瓶颈。
本研究采用混合方法评估了印度三个邦六个地区公共卫生机构的糖尿病护理服务。该研究描述了公共卫生机构提供的糖尿病护理服务,并确定了应对这些服务的挑战和解决方案。定量部分包括对服务和资源可用性的评估,而定性部分则包括对医疗服务提供者和糖尿病患者进行半结构化访谈,以了解护理途径。
共走访了30家卫生机构:5家三级医疗机构;8家中级医疗机构和17家初级卫生机构。这些机构未保存患者临床记录;患者有责任自行保存临床记录。所有机构都具备血糖测量设备,但糖化血红蛋白(HbA1c)检测仅在三级中心提供。三个邦的初级卫生中心均未提供HbA1c检测、血脂检查或足部护理。只有少数三级机构提供生活方式调整支持。大多数机构都有抗糖尿病药物(双胍类和磺脲类),且给药期限为14天。胰岛素和他汀类药物仅在二级和三级护理中心提供。共采访了42名医生,随访不佳、患者负担过重和缺乏专业培训是访谈中出现的主要障碍。共采访了37名患者。患者必须前往三级机构取药和进行常规随访,从而导致这些机构人满为患。没有正式的转诊或随访机制将患者与分散的机构联系起来。
有效的糖尿病管理实践与其实施之间存在很大差距。二级护理机构在随访调查和并发症筛查中应发挥更大作用。需要一个全面的糖尿病护理套餐,包括强大的记录和队列监测系统以及适当的转诊机制。