Deng Chao, Zhang Na, Wang Yapeng, Jiang Shun, Lu Min, Huang Yan, Ma Jin'an, Hu Chunhong, Hou Tao
Department of Oncology, the Second Xiangya Hospital, Central South University, Changsha, Hunan, China.
Medicine (Baltimore). 2019 Aug;98(33):e16875. doi: 10.1097/MD.0000000000016875.
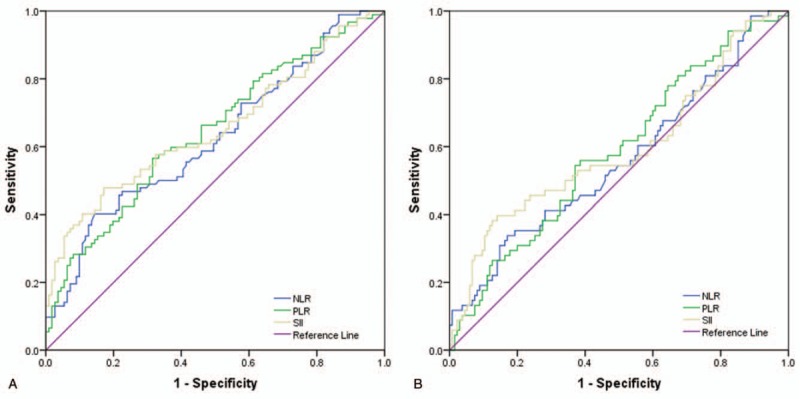
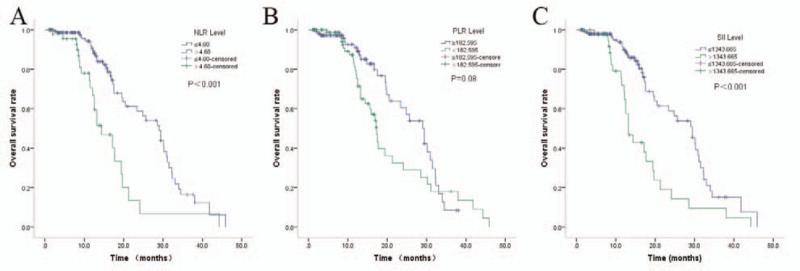
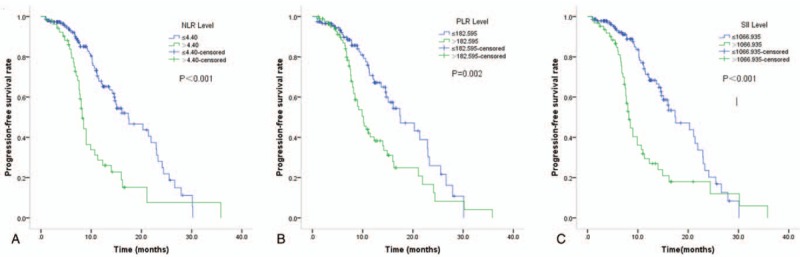
EGFR-TKIs have been widely used in the first-line treatment of NSCLC patients harboring EGFR mutations. However, the prognosis indicators are limited. In the present study, the prognostic value of systemic immune-inflammation index (SII), neutrophil to lymphocyte ratio (NLR), and platelet to lymphocyte ratio (PLR) were assessed in EGFR-Mutant lung adenocarcinoma patients treated with first-generation EGFR-TKIs. Two hundred three patients were included in this retrospective analysis. SII was calculated as platelet counts × neutrophil counts / lymphocyte counts. Receiver operating characteristic (ROC) curve was used to evaluate the optimal cut-off value for SII, NLR, and PLR. Univariate and multivariate survival analysis were performed to identify factors correlated with PFS and OS. Applying cut-offs of ≥1066.935 (SII), ≥4.40 (NLR), and ≥182.595 (PLR), higher NLR was associated with worse Eastern Cooperative Oncology Group performance status (ECOG PS) (P = .006), and higher brain metastasis rate (P = .03), higher PLR was associated with smoking history (P = .037), and worse ECOG PS (P = .001), and higher SII groups were associated with worse ECOG PS (P = .002). In univariate analysis, higher NLR (P < .001), higher PLR (P = .002), and higher SII (P < .001) were associated with worse PFS. Higher NLR (P < .001), and higher SII (P < .001) were associated with worse OS. In multivariate analysis, NLR (HR 1.736;95%CI:1.020-2.954; P = .03), PLR (HR 1.823; 95%CI:1.059-3.137; P = .04), and SII (HR2.577; 95%CI:1.677-3.958; P < .001) were independently correlated with PFS. While only SII (HR 2.802; 95%CI:1.659-4.733; P < .001) was independently correlated with OS. The present study demonstrated that SII is an independent prognostic factor for poor survival of advanced EGFR-Mutant lung adenocarcinoma patients treated with first-generation TKIs.
表皮生长因子受体酪氨酸激酶抑制剂(EGFR-TKIs)已广泛应用于表皮生长因子受体(EGFR)突变的非小细胞肺癌(NSCLC)患者的一线治疗。然而,预后指标有限。在本研究中,评估了全身免疫炎症指数(SII)、中性粒细胞与淋巴细胞比值(NLR)和血小板与淋巴细胞比值(PLR)在接受第一代EGFR-TKIs治疗的EGFR突变型肺腺癌患者中的预后价值。本回顾性分析纳入了203例患者。SII的计算方法为血小板计数×中性粒细胞计数/淋巴细胞计数。采用受试者工作特征(ROC)曲线评估SII、NLR和PLR的最佳截断值。进行单因素和多因素生存分析以确定与无进展生存期(PFS)和总生存期(OS)相关的因素。应用≥1066.935(SII)、≥4.40(NLR)和≥182.595(PLR)的截断值,较高的NLR与东部肿瘤协作组(ECOG)体能状态较差(ECOG PS)相关(P = 0.006),且脑转移率较高(P = 0.03),较高的PLR与吸烟史相关(P = 0.037),且ECOG PS较差(P = 0.001),较高的SII组与ECOG PS较差相关(P = 0.002)。在单因素分析中,较高的NLR(P < 0.001)、较高的PLR(P = 0.002)和较高的SII(P < 0.001)与较差的PFS相关。较高的NLR(P < 0.001)和较高的SII(P < 0.001)与较差的OS相关。在多因素分析中,NLR(风险比[HR] 1.736;95%置信区间[CI]:1.020 - 2.954;P = 0.03)、PLR(HR 1.823;95%CI:1.059 - 3.137;P = 0.04)和SII(HR 2.577;95%CI:1.677 - 3.958;P < 0.001)与PFS独立相关。而只有SII(HR 2.802;95%CI:1.659 - 4.733;P < 0.001)与OS独立相关。本研究表明,SII是接受第一代TKIs治疗的晚期EGFR突变型肺腺癌患者生存不良的独立预后因素。